
We’ve been here before – ‘wars’ on this and ‘wars’ on that. It’s strange how reluctant states are to admit that their use of military violence (especially when it doesn’t involve ‘boots on the ground‘) isn’t really war at all – ‘overseas contingency operations’ is what the Pentagon once preferred, but I’ve lost count of how many linguistic somersaults they’ve performed since then to camouflage their campaigns – and yet how eager they are to declare everything else a war.
These tricks are double-edged. While advanced militaries and their paymasters go to extraordinary linguistic lengths to mask the effects of their work, medical scientists have been busily appropriating the metaphorical terrain from which modern armies are in embarrassed retreat.
Yet all metaphors take us somewhere before they break down, and the ‘war on Ebola’ takes us more or less directly to the militarisation of the global response. In an otherwise critical commentary, Karen Greenberg draws parallels between the ‘the war on terror’ and the ‘war on Ebola’:
‘The differences between the two “wars” may seem too obvious to belabor, since Ebola is a disease with a medical etiology and scientific remedies, while ISIS is a sentient enemy. Nevertheless, Ebola does seem to mimic some of the characteristics experts long ago assigned to al-Qaeda and its various wannabe and successor outfits. It lurks in the shadows until it strikes. It threatens the safety of civilians across the United States. Its root causes lie in the poverty and squalor of distant countries. Its spread must be stopped at its region of origin — in this case, Guinea, Liberia, and Sierra Leone in West Africa — just as both the Bush and Obama administrations were convinced that the fight against al-Qaeda had to be taken militarily to the backlands of the planet from Pakistan’s tribal borderlands to Yemen’s rural areas.’
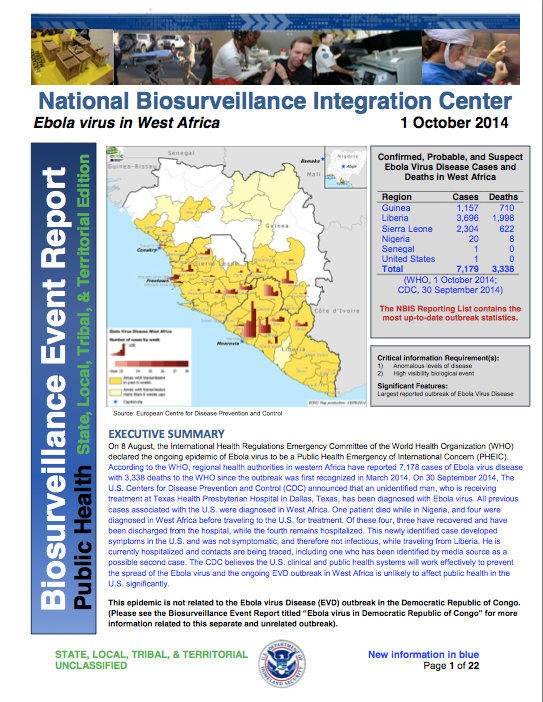
There are other parallels too, not least the endless re-descriptions of terrorism and even insurgency as life-threatening diseases, ‘cancers’ on the body politic. And, as Josh Holmes shows, there is also an entirely parallel (geo)politics of fear in both cases (see also Rebecca Gordon on the racialization of ‘the fear machine’ here). Given the threat supposedly posed by ‘the enemy within’, it’s not surprising that US Northern Command has already set up a 30-person ‘military rapid response team‘ for domestic Ebola cases, and that the Department of Homeland Security has been issuing Biosurveillance Event Reports on the Ebola outbreak in West Africa from the National Biosurveillance Integration Center.
But as I’ve said, Karen’s is a critical commentary and so, before the military metaphors carry us away, her conclusion bears repeating:
The United States is about to be tested by a disease in ways that could dovetail remarkably well with the war on terror. In this context, think of Ebola as the universe’s unfair challenge to everything that war bred in our governmental system. As it happens, those things that the U.S. did, often ineffectively and counterproductively, to thwart its enemies, potential enemies, and even its own citizenry will not be an antidote to this “enemy” either. It, too, may be transnational, originate in fragile states, and affect those who come in contact with it, but it cannot be stopped by the methods of the national security state.
To make sense of all this, I think we need to stand back and start with four general observations:
(1) Modern military medicine has long involved more than evacuating and treating the wounded from the field of battle. It has always had a substantial public health component. Until the early twentieth century, ‘infectious diseases unrelated to trauma were responsible for a much greater proportion of the deaths during war than battle-related injuries‘. As militaries started to pay much closer attention to hygiene and disease prevention, Matthew Smallman-Raynor and Andrew Cliff estimate that the ratio of ‘battle deaths’ to deaths from disease amongst the military population fell from 1:0.4 in the First World War to 1:0.1 in the Second World War; then it rose to 1:0.13 in the Vietnam War but in the first US-led Gulf War (1991) it fell to 1:0.01.
 (2) Modern militaries are no strangers to biowarfare either. Both sides in the First World War experimented with chemical weapons, and although the US Army’s explicitly offensive Biological Warfare Weapons Laboratories closed in 1969 the commitment to ‘bio-defense’ and bio-security has ensured a continuing military investment in the weaponisation of infectious diseases (see right). I don’t subscribe to the view that the Ebola epidemic in West Africa is the result of a rogue US biowarfare program – see for example the claims made by ‘Robert Wenzel’ here: and if you want to know why his name is in scare-quotes, appropriately enough, read Chris Becker‘s takedown here – nor to the fear that what Scientific American calls ‘weaponised Ebola’ is poised to become a ‘bio-terror threat’. But I do think it worth noting the work of the US Army Medical Research Institute of Infectious Diseases which has had field teams on the ground in West Africa since 2006, and the importance placed on surveillance and monitoring.
(2) Modern militaries are no strangers to biowarfare either. Both sides in the First World War experimented with chemical weapons, and although the US Army’s explicitly offensive Biological Warfare Weapons Laboratories closed in 1969 the commitment to ‘bio-defense’ and bio-security has ensured a continuing military investment in the weaponisation of infectious diseases (see right). I don’t subscribe to the view that the Ebola epidemic in West Africa is the result of a rogue US biowarfare program – see for example the claims made by ‘Robert Wenzel’ here: and if you want to know why his name is in scare-quotes, appropriately enough, read Chris Becker‘s takedown here – nor to the fear that what Scientific American calls ‘weaponised Ebola’ is poised to become a ‘bio-terror threat’. But I do think it worth noting the work of the US Army Medical Research Institute of Infectious Diseases which has had field teams on the ground in West Africa since 2006, and the importance placed on surveillance and monitoring.
(3) I also think it’s necessary to think through the biopolitics of public health in relation to military and paramilitary violence. This takes multiple forms. It’s become dismally apparent that in many conflict zones hospitals, doctors and other health-care workers have become targets: in Gaza, to be sure, but in Syria and elsewhere too. The treatment of disease has also become a tactical vector: think of the CIA’s use of polio vaccination campaigns as a cover for its intelligence operations and – the conjunction is imperative – the Taliban’s manipulation of polio vaccinations in Pakistan’s Federally Administered Tribal Areas. Think, too, of the way in which the Assad regime has inflicted a resurgent, even counterinsurgent geography of polio on the Syrian people. As Annie Sparrow shows (see also here):
‘This man-made outbreak is a consequence of the way that Syrian President Bashar al-Assad has chosen to fight the war—a war crime of truly epidemic proportions. Even before the uprising, in areas considered politically unsympathetic like Deir Ezzor, the government stopped maintaining sanitation and safe-water services, and began withholding routine immunizations for preventable childhood diseases. Once the war began, the government started ruthless attacks on civilians in opposition-held areas, forcing millions to seek refuge in filthy, crowded, and cold conditions. Compounding the problem are Assad’s ongoing attacks on doctors and the health care system, his besieging of cities, his obstruction of humanitarian aid, and his channeling of vaccines and other relief to pro-regime territory.

Late this summer she provided this update:
‘… nearly all the cases of polio have occurred in areas of northern Syria under rebel control, where the government is seemingly doing everything in its power to prevent vaccination. The Syrian government has appealed to the UN for hundreds of medicines for areas of the country it controls, while largely ignoring the far more dire needs of opposition-held areas. Many children, especially newborns, still do not have access to polio immunization. Daily government airstrikes target the very health facilities that should be the foundation of vaccination efforts, as well as the children who should be protected from polio, measles, and other preventable childhood diseases. As Dr. Ammar, a doctor from Aleppo, said to me bitterly after an April 30 airstrike killed twenty-two schoolgirls, “The government’s polio control strategy for children is to kill them before they can get polio.”’
(4) Finally, biopolitics threads its way from the sub-national and the national to the trans-national and so to what Sara Davies calls, in a vitally important essay, ‘securitizing infectious disease‘. (The link will take you to an open access version, which was originally published in International affairs 84 (2008) 295-313; see also her ‘The international politics of disease reporting: towards post-Westphalianism?‘, International politics 49 (2012) 591-613, and the collection she has edited with Jeremy Youde, The politics of surveillance and response to disease outbreaks: the new frontier for states and non-state actors – due out next year).
![]()
In her original essay, Sara shows how powerful states in the global North joined forces with the World Health Organisation to construct infectious disease as an existential security threat that demanded new rules and protocols for its effective containment. Crucially:
‘The outcome of this has been the development of international health cooperation mechanisms that place western fears of an outbreak reaching them above the prevention of such outbreaks in the first place. In turn, the desire of the WHO to assert its authority in the project of disease surveillance and containment has led it to develop global health mechanisms that primarily prioritizes the protection of western states from disease contagion.’
This has a genealogy as well as a geography (or what Alan Ingram once called a ‘geopolitics of disease’). Peter Dörrie notes that on 18 September 2014 the U.N. Security Council declared the current Ebola outbreak in West Africa ‘a threat to international peace and security’, and that this was ‘the first time the U.N. had taken this step in a public health crisis‘ (in fact the Council had previously expressed similar concerns about the impact of HIV/AIDS on ‘stability and security’). Under Chapter VII of the UN Charter this declaration has significant legal implications, as Jens David Ohlin notes here, but what most concerns Peter is how long it took for the Security Council to stir itself. It issued its statement 180 days after the WHO confirmed the outbreak, and over a month after the WHO had declared Ebola a ‘Public Health Emergency of International Concern’, and in his eyes the international system ‘ignored the problem until it was too big for any solution other than full-scale military intervention.’ But I’ve already suggested, it’s wrong to treat the militarisation of epidemic disease as somehow new. Of direct relevance to the present ‘war on Ebola’ is this passage from Sara’s essay:
The United States has been a keen participant in disease surveillance and response since the mid-1990s. The United States Department of Defense (US DoD) has had overseas infectious disease research laboratories located in over 20 countries for nearly ten years. The Global Emerging Infectious Surveillance and Response System (DoD-GEIS) mobile laboratories were set up for the purpose of ‘responding to outbreaks of epidemic, endemic and emergent diseases’, and their location in the DoD, as opposed to the United States Agency for International Development (USAID) or Centre for Disease Control (CDC) demonstrates how seriously the United States views the response to infectious disease as a key national security strategy.
So, four observations about the military-medical-security nexus that provide a context for the ‘war on Ebola’. There are two other issues that should also be on the table before proceeding.

The first involves the imaginative geographies circulating in the global North that (mis)inform public response to the epidemic. Many of them can be traced back to colonial descriptions of the coast of nineteenth-century West Africa (and Sierra Leone in particular) as ‘the white man’s grave’, a form of what in a different context Dan Clayton calls a ‘militant tropically’. The contemporary reactivation of these tropes is clearly a serious concern because it corrodes an effective political response. As geographer Kerrie Thornhill writes,
African and diaspora scholars, already accustomed to the ‘thousand tiny paper cuts’ of casual racism, demonstrate how these (metaphorical) cuts escalate into real fatalities. Writers such as Nanjala Nyabola and Lola Okolosie point out the abundance of racist tropes depicting West African societies as inherently unclean, chaotic, uncooperative, ungrateful, and childlike. This racism reinforces a global culture of disregard for black African lives, and the perception that they are a source of social and biological contamination.
You can find much more on this in Cultural Anthropology‘s brilliant Ebola in Perspective series.

The second is the precarious condition of health care systems in West Africa (Ebola in Perspective is good on this too). Brice de la Vigne, the operations director of MSF, reminds us that ‘both Sierra Leone and Liberia were at war ten years ago and all the infrastructure was destroyed. It’s the worst place on earth to have these epidemics.’ Other critics suggest that these uncivil wars were not the only culprits. In their view, it was the neoliberal economic model forced on West Africa by the global North that was primarily responsible for gutting public health systems:
While years of war played a role in weakening public systems, it is the “war against people, driven by international financial institutions” that is largely responsible for decimating the public health care system, eroding wages and conditions for health care workers, and fueling the crisis sweeping West Africa today, says [Emira] Woods. “Over the past six months to a year there have been rolling health care worker strikes in country after country—Nigeria, Sierra Leone, and Liberia,” said Woods. “Nurses and doctors are risking and losing their lives but don’t have protective gear needed to serve patients and save their own lives. They are on the front lines and have not had their voices heard.”

So – back to the front lines. Despite the geopolitical-military-security back story, it was Médecins Sans Frontières that made the first public call (on 2 September) for military assistance in combatting Ebola.
‘States with biological-disaster response capacity, including civilian and military medical capability, must immediately dispatch assets and personnel to West Africa…
‘Many countries possess biological threat response mechanisms. They can deploy trained civilian or military medical teams in a matter of days, in an organised fashion, and with a chain of command to assure high standards of safety and efficiency to support the affected countries…
‘In the immediate term, field hospitals with isolation wards must be scaled up, trained personnel must be dispatched, mobile laboratories must be deployed to improve diagnostics, air bridges must be established to move personnel and material to and within West Africa, and a regional network of field hospitals must be established to treat medical personnel with suspected or actual infections.’

Ten days later Peter Piot, the Director of the London School of Tropical Medicine and Hygiene and the microbiologist who helped identify the Ebola virus in 1976, also called for a ‘quasi-military intervention’. Although he spoke about a ‘state of emergency’, he too wanted to reverse the response prefigured by Giorgio Agamben in such situations and contract the spaces of exception that were multiplying across West Africa. He had in mind ‘beds, ambulances and trucks as well as an army of clinicians, doctors and nurses.’
What materialised was rather different.
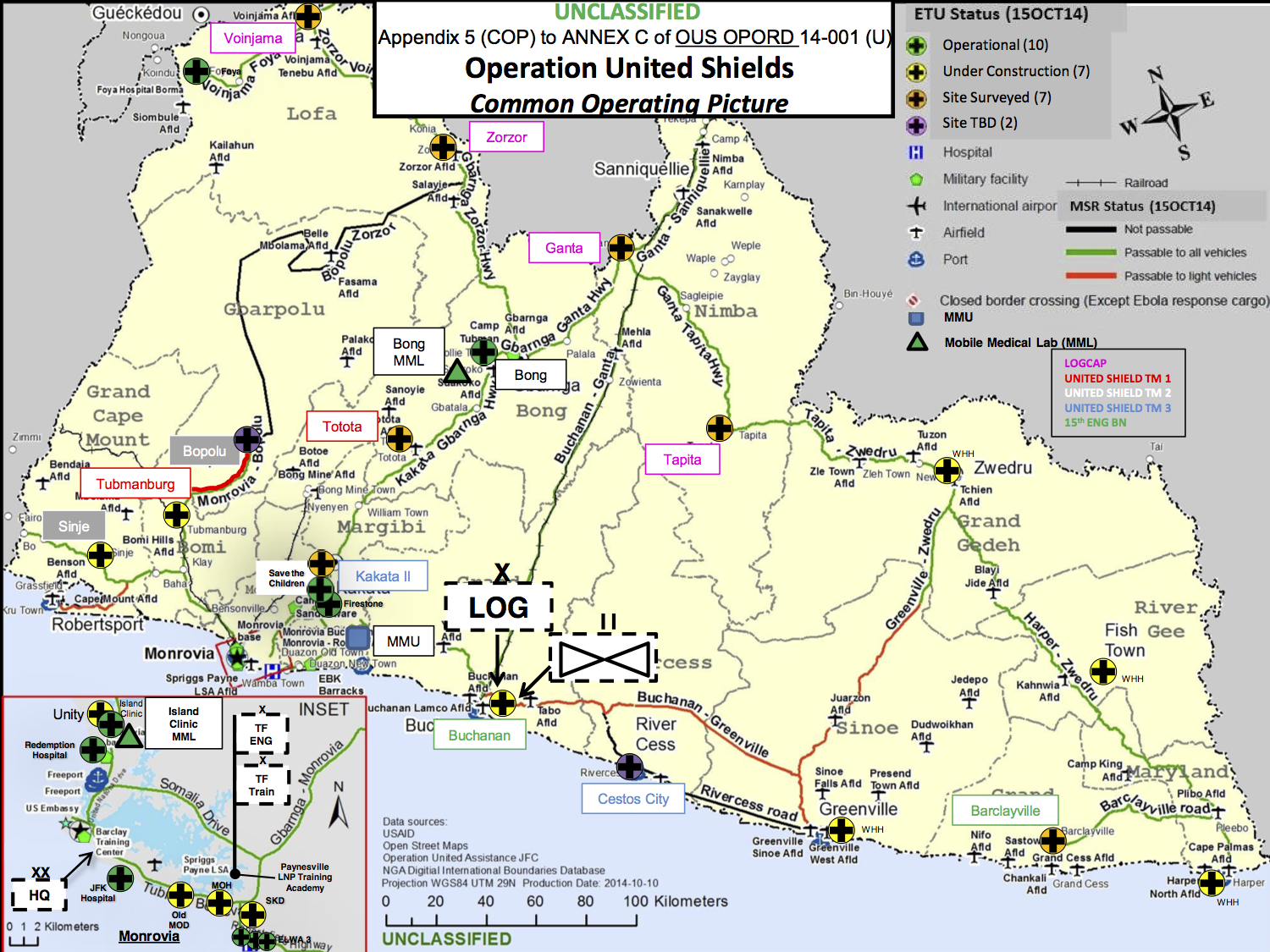
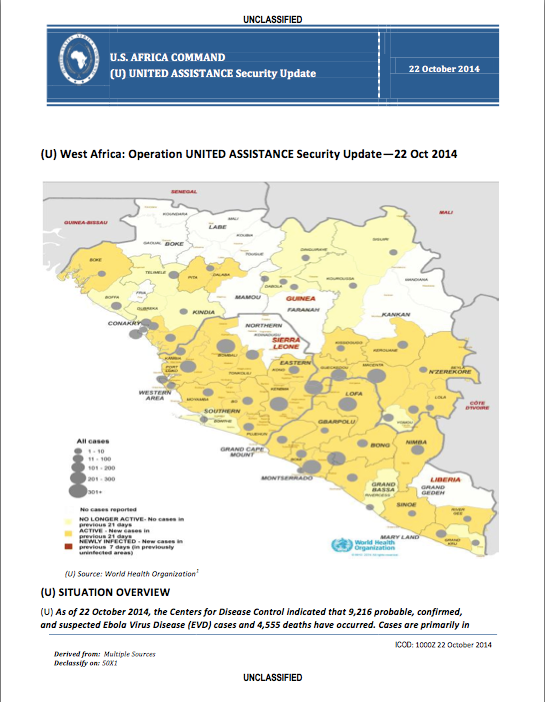
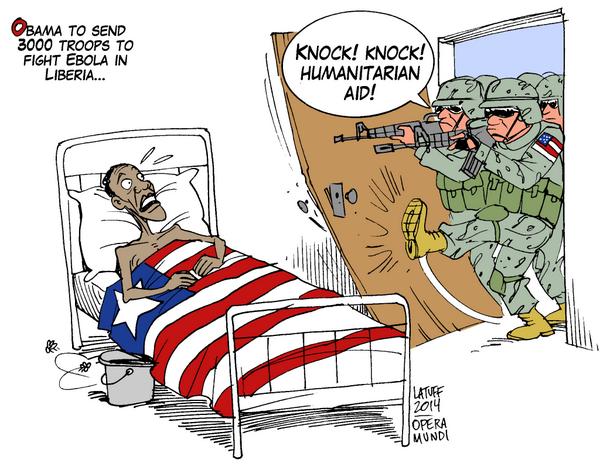
 On 16 September President Obama flew to the Centers for Disease Control and Prevention in Atlanta to announce Operation United Assistance. He committed 3-4,000 US troops and $750 million in defence funding to the mission, which is being orchestrated by US Africa Command (AFRICOM) through US Army Africa in concert with USAID. The focus of the US military-medical mission is Liberia. There are close historical connections between the US and Liberia, which originally offered to host AFRICOM’s headquarters in the capital Monrovia; now a Joint Force Command has been set up there. You can find the 75-page AFRICOM operational order here, dated 15 October 2014, from which I’ve taken the ‘common operating picture’ below. The title puzzles me – the only ‘Operation United Shield’ (singular) I’ve been able to find was a multinational operation to evacuate peacekeeping forces from Somalia in 1995. Appendix B is particularly worth reading, incidentally, because it identifies ‘the enemy’: ‘Ebola Virus Disease is the enemy, aided by poor preventive medicine practices in areas where EVD cases are prevalent and difficulties in identifying and treating EVD patients.’
On 16 September President Obama flew to the Centers for Disease Control and Prevention in Atlanta to announce Operation United Assistance. He committed 3-4,000 US troops and $750 million in defence funding to the mission, which is being orchestrated by US Africa Command (AFRICOM) through US Army Africa in concert with USAID. The focus of the US military-medical mission is Liberia. There are close historical connections between the US and Liberia, which originally offered to host AFRICOM’s headquarters in the capital Monrovia; now a Joint Force Command has been set up there. You can find the 75-page AFRICOM operational order here, dated 15 October 2014, from which I’ve taken the ‘common operating picture’ below. The title puzzles me – the only ‘Operation United Shield’ (singular) I’ve been able to find was a multinational operation to evacuate peacekeeping forces from Somalia in 1995. Appendix B is particularly worth reading, incidentally, because it identifies ‘the enemy’: ‘Ebola Virus Disease is the enemy, aided by poor preventive medicine practices in areas where EVD cases are prevalent and difficulties in identifying and treating EVD patients.’
The US deployment is complemented by the deployment of UK forces to Sierra Leone (Operation Gritrock)and French forces to Guinea. In both cases there are also close, colonial connections, and the British-led International Military Advisory Training Team Sierra Leone has been on the ground since 2000 (since last year this has been re-tasked as the International Security Advisory Team Sierra Leone).
(The map above is borrowed from the BBC; in addition, the Guardian has an interactive map tracing the historical geography of Ebola from the first known case in the Democratic Republic of Congo in 1976 to the present epidemic in West Africa here).
These forces differ in more than geographical deployment; their capabilities differ significantly too. The UK is sending 750 troops, including contingents from the Royal Army Medical Corps (notably 22 Field Hospital), who will construct treatment centres (the aim is to add 700 beds to triple Sierra Leone’s existing capacity) and treat doctors and other health-care workers who contract the disease; they are supported by the Royal Navy’s ‘Primary Casualty Receiving Ship’ RFA Argus (which will provide a further 100 beds), and by another 780 volunteer health care staff.
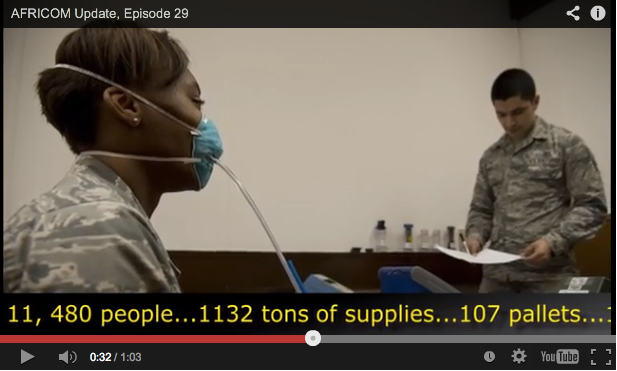
The US has mobilised troops from the 101st Airborne, whose primary mission is to set up 17 Ebola Treatment Units (each with 100 beds); meanwhile the US Air Force’s 633rd Medical Group is establishing a 25-bed Expeditionary Medical Support System field hospital for doctors and other health care workers who contract the disease (below). The US Army has also fielded three mobile laboratories to test samples for the virus, reducing the time to diagnosis from days to hours. According to Pardis Sabeti, who leads viral-genome research at the Broad Institute of M.I.T. and Harvard, ‘the faster you can get a diagnosis of Ebola, the faster you can stop it.’

‘Our enemy is a disease’, declared Lt Col Brian De Santis, echoing AFRICOM’s operational order – but it was quickly made clear that the vast majority of troops will not come into contact with the enemy or any of its victims at all. This is just as well; most of the soldiers have minimal medical training – just four hours from the US Army Medical Research Institute of Infectious Disease – and the Pentagon’s Press Secretary Rear Admiral John Kirby explained that there is ‘no intention right now that [troops] will interact with patients or be in areas where they would necessarily come into contact with patients’:
‘They’re not doctors. They’re not nurses. They’re not trained for that and not equipped for that. That’s not part of the mission. They will be kept in locations where they can do their jobs without coming into contact with patients.’
Andrew Bacevich thinks all this absurd:
‘It’s like the city that spends all its money to raise up a formidable police force only to discover that what it really needs is a bigger sewage treatment plant. Of course, you can always put cops to work burning human excrement but there are better — that is, more effective and cheaper — ways to solve the problem.’
In effect, this is another case of the military preferring remote operations. Here is a telling passage from Sophie Arie’s interview with MSF’s president Joanne Liu:
‘“Countries are approaching this with the mindset of going to war,” she says. “Zero risk. Zero casualties.” Liu describes the current military efforts as the equivalent, in public health terms, of airstrikes without boots on the ground. Pledges of equipment and logistical support are helpful—“The military are the only body that can be deployed in the numbers needed now and that can organise things fast.” But there is still a massive shortage of qualified and trained medical staff on the ground. “You need to send people not stuff and get hands on, not try to do this remotely,” Liu says…’
The primary areas for military operations in the ‘war on Ebola’ to date are surveillance, logistics and containment. I’ll consider each in turn.
Last week Public Intelligence released a series of weekly Security Updates and daily Intelligence Summaries produced by AFRICOM to support Operation United Assistance. These rely largely on WHO reporting to track the spread of the disease.
This is to work at a highly aggregate level. Most public health experts suggest that the key to stopping the spread of the disease is contact tracing – which, in its essentials, is the same methodology used by the military and the intelligence services to track individuals through terrorist and insurgent networks – and has been used successfully in both the United States and in Nigeria (which was declared free of Ebola on 20 October). Ezra Klein describes it as ‘almost ludicrously simple’ and ‘as low-tech as medicine gets’, and so it is in principle.
But its application in much of West Africa is immensely difficult: the UN estimates that only 16 out of 44 zones have adequate procedures and personnel in place. And since many local people are understandably fearful of the consequences of their answers, it is unlikely that military involvement would improve the situation. Here is Elizabeth Cohen and John Bonifield:
‘People are often uncooperative with the tracers, sometimes even throwing stones at health care workers. They fear that they or their loved ones will be put in the hospital; they’ve seen firsthand that people who go there often don’t return.
“The community perceives this as a death sentence,” [Donald Thea, an infectious disease epidemiologist] said. “Relinquishing your loved one is tantamount to death.”
And health care workers have very little to offer people as an incentive to cooperate. “With smallpox, we could offer people a vaccine, a carrot in essence to induce them to be cooperative. With Ebola, we have nothing,” Thea said.’
Logistics is the area where the military comes into its own. MSF had emphasised that its priorities included ‘the mass expansion of isolation centers, air bridges to move personnel and equipment to and within the most affected countries, mobile laboratories for testing and diagnosis, and building a regional network of field hospitals to treat suspected or infected medical personnel.’ Much of the military effort is currently concentrated in these areas, but the other side to mobilising medical personnel, equipment and testing and treatment facilities is, in effect, immobilising the population.
Containment runs the gamut from quarantine through curfews and lockdowns to border closures. Most observers believe that border closures would be counter-productive: if you want to know why, see Debora MacKenzie‘s short essay here. The other, seemingly lesser measures also have their dangers. In its original call for assistance, MSF insisted that ‘any military assets and personnel deployed to the region should not be used for quarantine, containment, or crowd control measures’, and it emphasised that ‘forced quarantines have only bred fear and unrest, rather than stem the virus.’
But others have other ideas. Major Matt Cavanaugh, from the US Army War College, has made an unofficial, back-of-the-envelope calculation of what a successful ‘containment strategy’ for Ebola would require. He is adamant that only ‘boots on the ground’ could do the job, though the nature of that ‘job’ remains elusive in his account. He talks about military logistics – the ability to ‘fix “the last mile” problem’ – but he also notes the need ‘to fill the basic state functions related to health, security, and public order in order to adequately respond to the threat.’ In case that triptych isn’t clear enough, in his subsequent ‘Ebola Manifesto‘ the major declares that ‘There is exactly one organization designed to rapidly hold and control territory and the people on it: the military.’ The figure he eventually arrives at – somewhere between 36,600 to 73,200 troops – is derived from the wars in Afghanistan and Iraq, and suggests that, for some commentators at least, the Ebola crisis is an opportunity to deepen AFRICOM’s investment in what Jan Bachmann calls ‘policing Africa’ [see his ‘Policing Africa: the US military and visions of crafting “good order”‘, Security Dialogue 45 (2) (2014) 119-36]:
‘The spectrum of [AFRICOM’s] activities can be understood most comprehensively through an analytical perspective of policing, in which the aim of establishing ‘good order’ through an expansive regulatory engagement in issues of welfare is applied to contexts of ‘fragile’ statehood and ‘ungoverned spaces’.’
This is not a uniquely American view. The Daily Mail (where else?) reports that one of the options being considered by Britain’s Chief of the General Staff is a full-scale military lockdown of Sierra Leone:
‘From a military perspective ebola is like a biological warfare attack and should be countered accordingly. There needs to be a clampdown on human movement inside Sierra Leone and possibly to and from the country between now and late 2015 when it is hoped that an antidote will have been developed.’
 It’s hard to know how much credence this should be given, of course, though the very existence of proposals like these suggests that the ‘soft power’ which Joeva Rock sees in the militarisation of Ebola conceals an iron fist. And Niles Williamson believes that the military-medical missions are a smokescreen:
It’s hard to know how much credence this should be given, of course, though the very existence of proposals like these suggests that the ‘soft power’ which Joeva Rock sees in the militarisation of Ebola conceals an iron fist. And Niles Williamson believes that the military-medical missions are a smokescreen:
‘The main purpose of this military operation is not to halt the spread of Ebola or restore health to those that have been infected. Rather the United States is seeking to exploit the crisis to establish a firm footing on the African continent for AFRICOM.’
That may be one of the objectives, but I think it’s a bridge too far to claim it as the main purpose: as I’ve tried to show, the militarisation and securitisation of Ebola has many other geopolitical and biopolitical dimensions. And Nick Turse has revealed that AFRICOM, far from having a ‘light footprint’, has already achieved a remarkably rapid tempo of operations across the whole continent.
Still, even in its less extreme versions, the ‘war on Ebola’ clearly raises urgent questions about the militarisation of humanitarian aid, about what Kristin Bergtora Sandvik calls a ‘crisis of humanitarian governance’, and about the violence that is involved in the production of the humanitarian present.

Pingback: Covid-19 and armed conflict | geographical imaginations
Pingback: A happier new year | geographical imaginations
Pingback: Fighting the War with the Ebola Drone | Norwegian Centre for Humanitarian Studies
Pingback: West Point and the war on Ebola | geographical imaginations
Pingback: Tomorrow’s Battlefield | geographical imaginations
Pingback: Countdown before midnight | geographical imaginations
Pingback: Fighting the War with the Ebola Drone, by Kristin B. Sandvik | Mats Utas
Pingback: Emergency Response | geographical imaginations
Pingback: Fighting Ebola | geographical imaginations
Pingback: Journeys from No Man’s Land | geographical imaginations
Reblogged this on Society for Radical Geography, Spatial Theory, and Everyday Life.
Reblogged this on Governing Emergencies and commented:
A great post by Derek Gregory on the metaphorical significance of ‘going to war’ on Ebola.
Reblogged this on Progressive Geographies and commented:
Derek Gregory discusses the militarised response to Ebola in a wide-ranging and well-referenced post.
The reading list I’ve been compiling on Ebola can be found here – http://wp.me/PUf6a-4yE