
Much of last week was taken up with working out a new project for the next round of the Social Science and Humanities Research Council’s Insight Grant programme. A ‘Notification of Intent’ to apply is required (I’m deliberately not saying ‘needed’) before you can actually apply in October – but since the NOI requires a plain-language summary and a figure for the total budget most of the planning has to be done months before the application. I could fill a whole blog – and other non-digital receptacles – about the sense in all that; suffice to say I hit the button ten seconds (sic) before the electronic shutters came down.
The application is for a project called Medical-Military Machines and the Casualties of War: Genealogies and Geographies of Care.

One of the central claims made by protagonists of later modern war is that its conduct is accurate and proportionate, legal and ethical, thereby raising the bar for ‘just’ or, as James Der Derian has it, ‘virtuous’ war (and as most readers will know, he would insist on those scare-quotes). It has done so, its advocates argue, by limiting casualties through new modes of intelligence, surveillance and reconnaissance, new weapons systems, and new modes of accountability. I explore these issues in my ongoing SSHRC project, Killing Space (DOWNLOADS tab) – not least through my continuing study of drones (much more to come!) – and this project maps its other, vitally important dimension – a sort of ‘Caring Space’ – in order to provide an indispensable substantive test for these claims.
The project concerns the provision of medical care for those wounded by military and paramilitary violence, casualties who are often overlooked in vexed but vital debates over ‘body counts’ and what constitutes (following Judith Butler) a grievable life. I’m not going to ignore those matters, far from it, but my main concern will be on the survivors of military violence. As I’ll explain in a moment, I want to analyse both combatant and civilian casualties, and so confound the simplistic politics in which the right is supposed to care about the one and the left about the other.
The project will involve both genealogy and geography. I’m using ‘genealogy’ in something like the Foucauldian sense, but all I’ll say here is that historical depth is plainly essential to specify what is (and is not) novel about the ways in which advanced militaries wage war. So the project will involve four case studies focusing on the United States and its allies. The first three are the Western Front in World War I, North Africa in World War II, and South Vietnam (1963-1975) . In this traverse from ‘total war’ to James Gibson’s ‘techno-war’ I’m planning to leverage my work on ‘The natures of war’. While researching that presentation and long-form essay – which will eventually appear in War Material – I found a treasure-trove of sources that I want to explore in much more depth and detail for this new project. The fourth case study will involve the cluster of wars in the Greater Middle East post 9/11, and while much of this has been familiar ground for me ever since I started writing The colonial present, there are many new issues to address – including the deliberate targeting of hospitals and medical doctors by some factions and what Omar Dewachti calls the ‘therapeutic geographies’ involved in the transnational movement of war casualties from (say) Iraq, Libya and Syria to hospitals in Lebanon, Jordan and India.
The project has three components that address different geographies of casualty care.

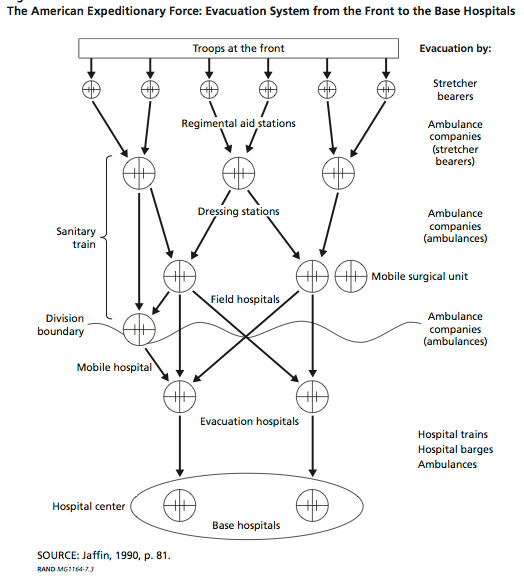
 (1) Modern military medicine has sought to provide immediate care for troops injured in combat as close to the site of the injury as possible by deploying medical personnel and equipment in forward positions, and establishing evacuation routes for more seriously injured patients to higher-order medical facilities in the rear. These systems have been transformed by technical advances designed to increase the time-space compression of treatment: the more widespread use of motorized ambulances in the Western Desert, for example, and helicopters for medical evacuation (‘dust-off’) in Vietnam and later conflicts. I plan to reconstruct these networks and their transnational extensions and to calibrate the changing transit times, and then to turn these skeletal geometries into human geographies through diaries, letters and, as we near the present, interviews, that I hope will bring into view the multiple people involved in these precarious, fleshy, and profoundly intimate journeys. My inspiration for this is a series of thought-provoking essays in the Journal of the Royal Army Medical Corps (really), which provide a way in to the geometries and networks, and (very different) Emily Mayhew‘s Wounded: from Battlefield to Blighty, 1914-1918, due out next month, which uses the idea of a ‘journey’ in what could develop into a sort of phenomenology of care; I’ll say some more about some of this in a later post.
(1) Modern military medicine has sought to provide immediate care for troops injured in combat as close to the site of the injury as possible by deploying medical personnel and equipment in forward positions, and establishing evacuation routes for more seriously injured patients to higher-order medical facilities in the rear. These systems have been transformed by technical advances designed to increase the time-space compression of treatment: the more widespread use of motorized ambulances in the Western Desert, for example, and helicopters for medical evacuation (‘dust-off’) in Vietnam and later conflicts. I plan to reconstruct these networks and their transnational extensions and to calibrate the changing transit times, and then to turn these skeletal geometries into human geographies through diaries, letters and, as we near the present, interviews, that I hope will bring into view the multiple people involved in these precarious, fleshy, and profoundly intimate journeys. My inspiration for this is a series of thought-provoking essays in the Journal of the Royal Army Medical Corps (really), which provide a way in to the geometries and networks, and (very different) Emily Mayhew‘s Wounded: from Battlefield to Blighty, 1914-1918, due out next month, which uses the idea of a ‘journey’ in what could develop into a sort of phenomenology of care; I’ll say some more about some of this in a later post.
The other two components follow from a remark made by Michel Foucault in ‘The Eye of Power’. There he suggested that ‘doctors, along with the military, were the first managers of collective space’, but he assigned them to different spaces (‘campaigns’ versus ‘habitations’). Instead I want to explore what happens when military and medicine are called upon to imagine and manage the same space and install what, following the example of Mark Harrison, I’m calling a ‘medical-military machine’ in a war-zone. So I’ll be following two tracks that are usually kept separate – civilian and combatant casualties (and here I want to extend the ongoing debates over their distinction from an abstract legal to a substantive therapeutic terrain) – and tracing the junctions where they intersect, in order to establish two other, complementary and sometimes countervailing geographies of care.

(2) There is an important sense in which modern war has always been ‘war amongst the people’: this is not a late twentieth-century preoccupation. Images of ‘No Man’s Land’ on the Western Front distract attention from the injuries suffered by civilian populations who continued to inhabit houses and work farms behind the front lines, for example, while ground and air offensives in South Vietnam produced hundreds of thousands of civilian casualties. So a second question is this: in what ways and in what places have militaries assumed medical responsibility for civilian casualties before and beyond the parameters of the Medical Civic Action Programs of contemporary counterinsurgency?

 (3) Conversely, the military has not been the only agency making medical interventions in war-zones, and this is not a late twentieth century development either. Civilian hospitals are increasingly important in today’s urban wars (where they often become targets too), but I want to pay particular attention to the work of international agencies. I plan to analyse two voluntary organisations, the Friends’ Ambulance Unit and the American Field Service in the two world wars, and (I hope) two contemporary NGOs, the most obvious candidates being the International Committee of the Red Cross and Médecins sans Frontières. I’m not assuming any direct filiations, and I’ll no doubt find all sorts of differences between them (particularly between the earlier and the later ones), but I’m particularly interested in the tensions between what at the moment I see as a common, more or less cosmopolitan engagement and the imperative to provide place-specific casualty care (and the logistics of doing so). So a third question revolves around the rise of a ‘militarized humanism’ and the emergence of what Didier Fassin calls ‘humanitarian reason’ as, perhaps, a form of governmentality.
(3) Conversely, the military has not been the only agency making medical interventions in war-zones, and this is not a late twentieth century development either. Civilian hospitals are increasingly important in today’s urban wars (where they often become targets too), but I want to pay particular attention to the work of international agencies. I plan to analyse two voluntary organisations, the Friends’ Ambulance Unit and the American Field Service in the two world wars, and (I hope) two contemporary NGOs, the most obvious candidates being the International Committee of the Red Cross and Médecins sans Frontières. I’m not assuming any direct filiations, and I’ll no doubt find all sorts of differences between them (particularly between the earlier and the later ones), but I’m particularly interested in the tensions between what at the moment I see as a common, more or less cosmopolitan engagement and the imperative to provide place-specific casualty care (and the logistics of doing so). So a third question revolves around the rise of a ‘militarized humanism’ and the emergence of what Didier Fassin calls ‘humanitarian reason’ as, perhaps, a form of governmentality.
This really is just a bare-bones summary, and since I have another two months to flesh it out I’d really welcome any advice, suggestions or criticisms. As I’ve described the project here you can see, I hope, that my case-studies and the questions I think they’ll enable me to address arise at the intersections of medical and military geography but also involve political, cultural and legal geographies. And, as ever, those geographies all have a stubbornly little g: this really isn’t a disciplinary project.

Pingback: A heavy reckoning | geographical imaginations
Pingback: War and demise | geographical imaginations
Pingback: War and therapeutic geographies | geographical imaginations
Pingback: When soldiers fall | geographical imaginations
Pingback: A mile in these shoes | geographical imaginations
Pingback: The Logistics of Evacuation | rhulgeopolitics
Pingback: Survivable life | geographical imaginations
Pingback: Medical-military machines and the casualties of war 1914-2014 | geographical imaginations
Pingback: A different sort of hell | geographical imaginations