This fall Middle East Report – described by Rashid Khalidi as ‘the best periodical (in English) on the Middle East—bar none’ – from the truly outstanding Middle East Research and Information Project became open access..\
Health and health care have become increasingly ungoverned over the past few decades, in tandem with a broader breakdown of the body politic. Health care workers are finding it increasingly difficult to work in settings of violent conflict and insecurity, rapidly declining health care systems, pervasive corruption and widespread economic mismanagement—all amidst the waning capacity of states to improve the health and wellbeing of their populace. While the Middle East region trains a lot of doctors, few end up staying. The winter issue of Middle East Report explores the interactions of the body politic with health and medicine and examines the entanglements of physical bodies in the institutional and political processes that govern them. The articles in this issue explore a range of different landscapes and ecologies of politics and health care, bringing the questions and problems of health and illness into the analysis of geopolitics and political economy.
Contents:
The Evolution of Conflict Medicine in the Middle East – An Interview with Ghassan Abu Sittah Ghassan Abu Sittah, Omar Dewachi, Nabil Al-Tikriti The Long Shadow of Iraq’s Cancer Epidemic and COVID-19 Mac Skelton Syrian Refugees Navigate Turkey’s Shifting Health Care Terrain Nihal Kayali Hepatitis C, COVID-19 and the Egyptian Regime’s Approach to Health Care Jennifer Derr The Dilemmas of Practicing Humanitarian Medicine in Gaza Osama Tanous Illness as Metaphor and Reality in Syria Noura Chalati COVID-19 Exposes Weaknesses in Syria’s Fragmented and War-Torn Health System Aula Abbara
The next installment of ‘Under Afghan Skies‘ will appear this week, but I’ve also been trying to pull together what information and insight there is on the impact of the pandemic on Syria (more on that soon too). En route, these more general reflections provide some helpful context:
(A) International Crisis Group on Covid-19 and conflict: seven trends to watch is here. This was written late last month, and it’s clearly a rapidly evolving situation, but in brief the trends identified by the ICG are:
(1) The vulnerability of conflict-affected populations
‘The populations of conflict-affected countries – whether those in war or suffering its after-effects – are likely to be especially vulnerable to outbreaks of disease. In many cases, war or prolonged unrest, especially when compounded by mismanagement, corruption or foreign sanctions, have left national health systems profoundly ill-prepared for COVID-19… The areas of active conflict at highest immediate risk of COVID-19 outbreaks may be north-western Syria, around the besieged enclave of Idlib, and Yemen. Both countries have already experienced health crises during their civil wars, with violence impeding the international response to an outbreak of polio in Syria in 2013-2014 and cholera in Yemen from 2016 onward. UN officials have now raised the alarm about COVID-19 infecting the population of Idlib, where a Russian-backed offensive by government forces has systematically targeted hospitals and other medical facilities and led to the displacement of over one million people in the last six months alone. Many people fleeing clashes sleep in fields or under trees, and basic hygiene and social distancing practices are made impossible by the lack of running water or soap as well as cramped living spaces….
Also of concern are the Rohingya refugee camps in Bangladesh, where over one million people live in overcrowded conditions, with sanitation facilities and health care services limited to a bare minimum. A government ban on internet and mobile phone services in the camps limits access to vital preventive information, while high levels of malnutrition likely imply that both the refugees and local residents are more susceptible to the disease. Should COVID-19 reach the camps, humanitarian agencies expect it to spread like wildfire, potentially triggering a backlash from Bangladeshis who live in the surrounding areas and are already unnerved by the refugees’ prolonged stay.
In these cases – as for displaced communities in Iraq and elsewhere in the Middle East, Africa and Asia – there is a risk that IDPs and refugees facing large-scale outbreaks of COVID-19 in the camps where they reside may aim to flee again to safety, leading local populations or authorities to react forcefully to contain them, which creates the potential for escalating violence. States attempting to stop the spread of the disease are likely to view new refugee flows fearfully. Colombia and Brazil, for example, closed their borders with Venezuela after previously taking a relatively generous approach to those fleeing the crisis there, but the pressure to escape worsening poverty and health risks in Venezuela could force rising numbers of migrants to use illegal crossings.’
(2) Damage to international crisis management and conflict resolution mechanisms
‘One reason why refugee and IDP populations are likely to be especially vulnerable to COVID-19 is that the disease could severely weaken the capacity of international institutions to serve conflict-affected areas. WHO and other international officials fear that restrictions associated with the disease will impede humanitarian supply chains. But humanitarian agencies are not the only parts of the multilateral system under pressure due to the pandemic, which is also likely to curb peacemaking.
Travel restrictions have begun to weigh on international mediation efforts. UN envoys working in the Middle East have been blocked from travelling to and within the region due to airport closures. Regional organisations have suspended diplomatic initiatives in areas ranging from the South Caucasus to West Africa, while the envoy of the International Contact Group on Venezuela – a group of European and Latin American states looking for a diplomatic solution to the crisis there – had to cancel an already long-delayed trip to Caracas in early March for COVID-related reasons.
The disease could affect crucial intra-Afghan peace talks planned as a follow-up to the February preliminary agreement between the U.S. and the Taliban, at least reducing the number of those who can participate (although limiting the group to real decision-makers and essential support staff could be conducive to serious talks).
More broadly, the disease means that international leaders, focused as they are on dramatic domestic issues, have little or no time to devote to conflicts or peace processes…
The disease could also affect multinational peacekeeping and security assistance efforts. In early March, the UN secretariat asked a group of nine peacekeeping troop contributors – including China and Italy – to suspend some or all unit rotations to blue helmet operations due to concerns about the spread of COVID-19. UN operations have announced further limits to rotations since then, meaning that peacekeepers’ tours of duty will be extended for at least three months in tough mission settings such as the Central African Republic and South Sudan, potentially affecting their morale and effectiveness.’
(3) Risks to social order
‘COVID-19 could place great stress on societies and political systems, creating the potential for new outbreaks of violence. In the short term, the threat of disease is likely acting as a deterrent to popular unrest, as protesters avoid large gatherings. COVID-19’s emergence in China precipitated a decline in anti-Beijing protests in Hong Kong (although public discomfort with radical elements of the protest movement may also have been a factor). There has been a decline, too, in the numbers of protesters taking to the streets in Algeria to challenge government corruption. The Russian opposition largely acquiesced in the authorities’ move, ostensibly justified on health grounds, to block protests against President Vladimir Putin’s decision to rewrite the constitution to extend his tenure in office. At least one exception to this general caution occurred in Niger, where demonstrators took to the streets against rules barring protest, which the government extended by invoking COVID-19. Three civilians were killed by security forces on 15 March.
Yet the quiet in the streets may be a temporary and misleading phenomenon. The pandemic’s public health and economic consequences are liable to strain relations between governments and citizens, especially where health services buckle; preserving public order could prove challenging when security forces are overstretched and populations become increasingly frustrated with the government’s response to the disease….
More broadly, the disease’s catastrophic economic impact could well sow the seeds of future disorder. It could do so whether or not the countries in question have experienced major outbreaks of the disease, although the danger in those that have will be magnified. A global recession of as yet unknown scope lies ahead; pandemic-related transport restrictions will disrupt trade and food supplies; countless businesses will be forced to shut down; and unemployment levels are likely to soar.’
(4) Political exploitation of the crisis
‘Against this background of social pressures, there is ample room for political leaders to try to exploit COVID-19, either to solidify power at home or pursue their interests abroad…. Nonetheless, as the crisis goes on, some leaders could order restrictive measures that make public health sense at the peak of the crisis and then extend them in the hope of quashing dissent once the disease declines. Such measures could include indefinite bans on large public gatherings – which many governments have already instituted to stop community spread of COVID-19 – to prevent public protests. Here again there are precedents from West Africa’s Ebola crisis: local civil society groups and opposition parties claim that the authorities prohibited meetings for longer than necessary as a way of suppressing legitimate protests. A harbinger of what is to come may have appeared in Hungary, where Prime Minister Viktor Orban asked parliament on 21 March to indefinitely extend a state of emergency that prescribes five-year prison sentences for those disseminating false information or obstructing the state’s crisis response….
… the crisis may create openings for jihadist groups to launch new offensives against weakened governments in Africa and the Middle East. To date, neither ISIS nor any of al-Qaeda’s various branches has displayed a clear strategic vision relating to the pandemic (although ISIS has circulated health guidance to its militants on how to deal with the disease based on sayings by the Prophet Muhammad).’
(5) A turning-point in major power relations?
‘The potential effects of COVID-19 on specific trouble spots is magnified by the fact that the global system was already in the midst of realignment…
In 2014, the U.S. took charge of a belated multilateral response to the West Africa Ebola crisis helped by countries ranging from the UK and France to China and Cuba. Today, the U.S. – whose international influence already had considerably weakened – has simultaneously mishandled its domestic response to COVID-19, failed to bring other nations together and stirred up international resentment. President Donald Trump has not only harped on the disease’s Chinese origins but also criticised the EU for bungling its containment.
China, by contrast, after having to cope with the consequences of the initial outbreak, its early and costly decision to hold back information, and its own uneven response, and having sought at times to blame the U.S. by waging an irresponsible misinformation campaign, now sees in the health crisis an opportunity to gain influence over other states through humanitarian gestures’.
(6) Opportunities to be siezed
‘While the warning signs associated with COVID-19 are significant, there are also glimmers of hope. The scale of the outbreak creates room for humanitarian gestures between rivals. The UAE has, for example, airlifted over 30 tonnes of humanitarian aid to Iran to deal with the disease (Bahrain, by contrast, took the opportunity to accuse the Islamic Republic of “biological aggression”).
(7) Potential crisis mitigation measures
‘Looking ahead, governments will have to decide whether to support more cooperative approaches to handling the crisis, not only in global public health terms but also as a political and security challenge. All leaders face pressure to focus on and spend money and political capital on domestic priorities, and in particular to ignore conflict risks in weak states that may seem hard to resolve or simply not important enough to worry about. But there will be a day after, and if the coming period is not dealt with wisely, it could be marked by major disruptions in already conflict-ridden areas, the eruption of new violence and a far more fragile multilateral system…. The COVID-19 pandemic threatens to be long and draining. It will make diplomacy, and especially crisis diplomacy, harder. But it is crucial to keep channels of communication – and a spirit of cooperation – intact in a period when the international system seems as ready as ever to fragment.’
(B) International Committee of the Red Cross: Cordelia Droege‘s post on ‘COVID-19 response in conflict zones hinges on respect for international humanitarian law‘ is here.
‘…the extreme vulnerability of people in conflict zones to COVID-19, the culmination of degraded or collapsed essential services such as water, sanitation, and health care, is in significant part the result of a disregard over many years of States’ and other belligerents’ obligations – as set out in international humanitarian law and international human rights law – towards populations under their control.
Now we are here, at a new crossroads, but one with familiar signposts. In the long term, a public health response to a pandemic and respect for fundamental legal protections go hand in hand. To illustrate this, the ICRC Legal Division has produced a basic reminder of the key provisions of international humanitarian law, relevant to the COVID-19 pandemic in conflict situations, that we must all keep close at hand when a pandemic hits countries at war.’
She then lists in clear, summary form those key IHL provisions (which concern both rights and responsibilities) in relation to:
Medical personnel, provisions and transport
Water supply
Humanitarian relief
Persons specifically at risk
Detainees
Internally displaced persons, migrants, asylum seekers and refugees
Children and education
Sanctions regimes and other restrictive measures
(C)Christine Bell has another helpful post over at Just Security on ‘COVID-19 and Violent Conflict: Responding to Predictable Unpredictability‘ here.
She draws on ongoing research from the Political Settlements Research Programme to identify ‘baseline understandings are likely to be key in designing the most effective responses to the COVID-19 pandemic in conflict-affected regions.’
The PS Research Programme also has a useful list of resources on Conflict, Development and Covid-19here.
(D) In a previous series of posts I discussed the militarized response to Ebola – see here, here and here – and Diana Ojeda and Lina Pinto García have provided a chilling, illuminating commentary from Colombia on ‘The militarization of life under war, “post-conflict,” and the COVID-19 crisis‘ here.
(E) Finally – essentially – three thoughtful reflections on the dangerous work done by deploying (sic) the rhetoric of war to discuss the novel Coronavirus (see also my post here):
Eve Fairbanks, ‘A pandemic is not a war‘, at HuffPosthere;
Adriano Iaria, ‘We are not at “war” with COVID-19: concerns from Italy’s “frontline”‘, at ICRC’s Humanitarian Law and Policy blog here;
Federica Caso, ‘Are we at war? The rhetoric of war in the Coronavirus pandemic‘, at The Disorder of Thingshere.
We know how often the vocabulary of medicine has been hi-jacked to describe military violence (‘surgical strikes’ and the rest) – if you are unfamiliar with the trope, I recommend Colleen Bell’s two essays, ‘Hybrid warfare and its metaphors’, Humanity 3 (2) (2012) 225-247, and ‘War and the allegory of medical intervention’, International Political Sociology 6 (3) (2012) 325-8 – and, for that matter, the reverse: see Mark Harrison‘s classic essay, ‘The medicalization of war – the militarization of medicine’, Social History of Medicine 9 (2) (1996) 267–276.
The most obvious example of the latter is Trump’s grotesque self-inflation as a ‘war-time president‘ defeating the ‘Chinese virus’ (the racialization of epidemic disease has a long history too: think of European panic over the ‘Asiatic’ or ‘Indian cholera’ in the nineteenth century). Another example, grotesque for entirely other reasons – which have to do with the mendacious incompetence of the US feral government – are descriptions of scenes in hospitals in New York City as war-zones where front-line doctors and nurses desperately struggle to treat and care for patients with Covid-19 while fighting for their own lives. (For brief but insightful commentaries on these issues, on the performative work done by these metaphors, see Yasmeen Serhan at The Atlantichere and Eric Levenson at CNN here).
None of this is confined to the United States, I realise, and the questions that swirl through these metaphors (through which the virus becomes both a biopolitical and a social agent, infecting not only bodies and populations but also our imaginative geographies) reappear in still starker form once we think – in obdurately non-metaphorical terms – about the likely course of Covid-19 in war zones like Gaza, Iraq, Syria and Yemen where hospitals and clinics have been deliberately and systematically targeted, doctors and nurses killed, and the lives of desperately vulnerable populations inside and outside refugee camps made even more precarious (I’ll try to address this in detail in a later post, but see here and here).
All this is on my mind, a jumbled series of thoughts, impressions and emotions, as I sit at home – privileged and relatively safe – doing my best to practice physical distancing, and read this imaginative call for contributions from Warscapes.
We find ourselves in a truly challenging moment as this coronavirus pandemic becomes a long and difficult daily reality. Not only are our individual lives feeling severely compromised but the massive structural shifts are beyond despairing — the shocking death toll, the triumph of surveillance structures, the displacements, the police brutality, curfews, imminent starvation, mass unemployment…the list is long. We know that many of you have survived war, reported on war or lived through intensive periods of violence, scarcity and uncertainty. Perhaps you find yourself working through tangled memories of all kinds of warscapes. Perhaps some of you have no luxury of memory and have been thrown into the pandemic as doctors, social workers, aid workers, teachers, activists. Perhaps some of you have seen this as a welcome respite from a deeply pressured life and are enjoying time with family. Perhaps some are in an intellectual overdrive as our fight against inept governments and greedy capitalist systems intensifies. And perhaps some of you are quite ill and we wish you love and speedy healing. Whatever mood or situation you find yourself in, we are somehow all in this together processing our new reality, wittingly or unwittingly.
Unsurprisingly, there is an uptick in war rhetoric during this pandemic and since this is an online space dedicated to reflecting on the world through the “lens of war” we are launching a Warscapes video segment tentatively titled “Open Call: The Corona Notebooks.” If you are willing and able, we would love it if you could record a 2-3 minute video of yourself thinking about this pandemic, maybe accessing a previous memory, maybe reporting on an injustice, maybe narrating a sweet fragment from your daily life, maybe recounting a second chance that this pandemic gave you, maybe telling us about a loved one you reconnected with, maybe you’ve seen a movie or read a book that was powerful, maybe telling us about having the illness. The tone, the tale, the genre and the language is yours to choose. There is an overwhelming amount of news and information but we will together weave an emotionally vibrant and artistic tapestry.
We will simultaneously transcribe these and start publishing them online as well. And when/if/after this is all over, we can publish all the entries and either give them away as free chapbooks or see if it can go towards a relief effort. For those that are available and happy to do facebook/instagram live events, we will happily make this an event with audience interaction and allow for discussions centering around your piece.
Simple rules:
1. WIDESCREEN recording — Flip your phone to widescreen. Do NOT shoot in vertical.
2. CLEAR SOUND — Make sure the sound is clear, our world has been quiet so this should be easy.
3. PLAN IN ADVANCE — While informal, casual and intimate is great, it would be better write your piece down, work through it before recording, experiment with form, play with the visual. We would prefer to keep editing to the minimal.
4. TWO MINUTES MINIMUM — your entry should be at least 2 minutes long, no stipulations for maximum length.
5. Send videos to bhakti [dot]shringarpure[at]gmail [dot]com
If you too are sitting at home, weary of yet another Zoom meeting, and wondering what (else) you might do, then perhaps you might like to give this a try…
For Sama – see my posts here and here – is now available on YouTube:
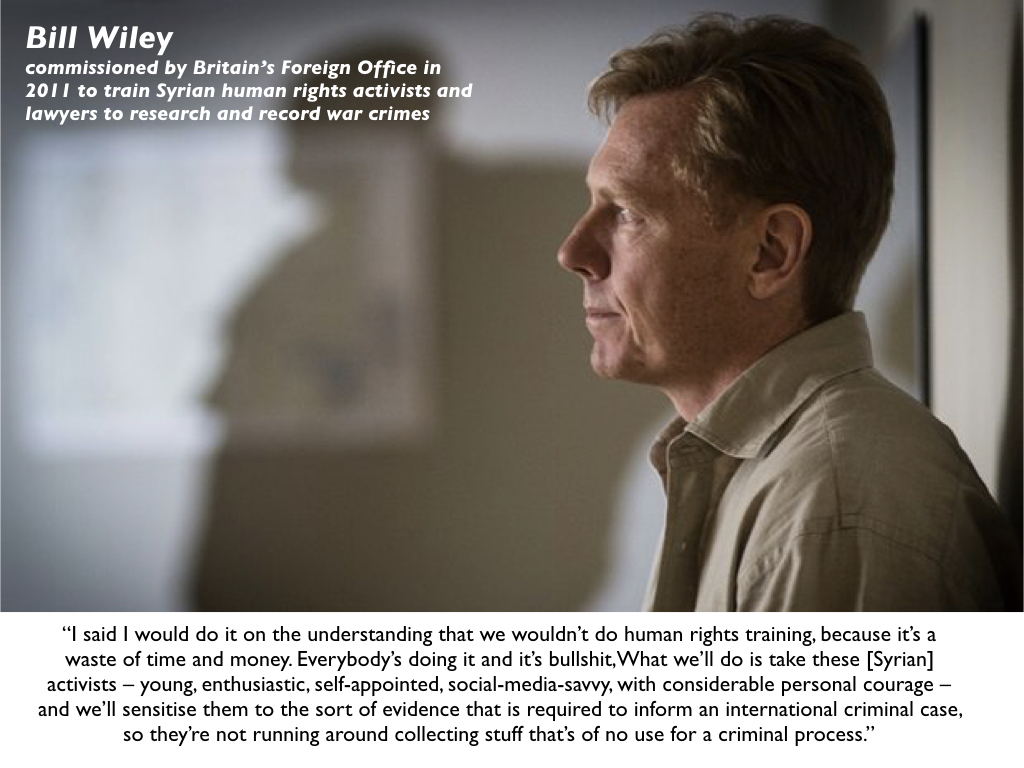
Sama is the daughter of the film-maker Waad al-Kateab and her husband Hamza, a hospital doctor and one of 32 who remained in East Aleppo.
For Sama was shot in East Aleppo; it begins in the early days of the rising against the Assad regime and focuses on life in and around two hospitals during the siege.
‘Sama’, we are told,
‘means the sky…. the sky we love, the sky we want… without airforces, without bombing… the sky with sun, with clouds, with birds…’
After their original hospital was destroyed in an airstrike – one of the doctors killed was Muhammad Waseem Maaz, who had delivered Sama (see also here and the slides for Death of the Clinic under the TEACHING tab) – they were able to move to a building ‘designed to be a hospital’ but never used and ‘not on any maps so the Russians and the regime wouldn’t know where to bomb…’
It would be the last hospital left functioning in East Aleppo, treating almost 300 patients a day.
‘Even when I close my eyes I see the colour red. Blood everywhere. On walls, floors, our clothes. Sometimes we cry blood.’
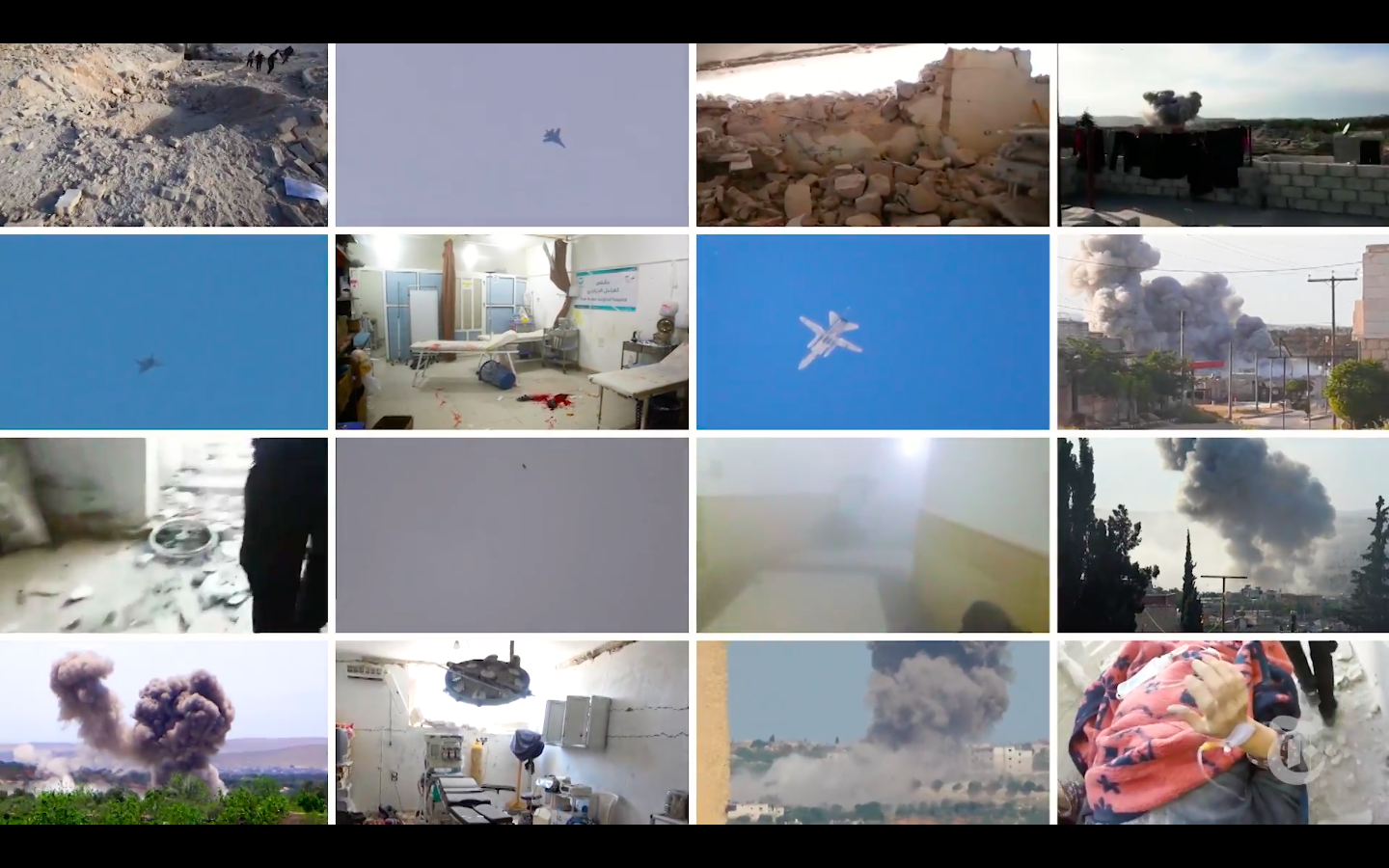
There is a stunning report (including an extended video) in today’s New York Times providing detailed evidence of Russian jets systematically attacking four hospitals in Syria in just twelve hours on 5/6 May 2019.
As regular readers will appreciate, this is a fraction of the total number of attacks on hospitals and clinics by Russian and Syrian aircraft – see my analysis in ‘Your turn, doctor’ here, ‘Death of the Clinic’ here and a stream of subsequent posts.
There have been other attempts to attribute culpability in the past – I’m thinking here of visual analysis by bellingcat and Forensic Architecture, for example – and, as the NYT notes, ‘recklessly or intentionally bombing hospitals is a war crime, but proving culpability amid a complex civil war is extremely difficult, and until now, Syrian medical workers and human rights groups lacked proof.’ What distinguishes this (brilliant) investigation is the incorporation of flights logs and intercepts of radio communications from the Russian Air Force that for the first time clearly and unambiguously show that these air strikes were deliberate, systematic and relentless attacks on known hospitals.
Here is the first attack analysed by the NYT; I’ve grabbed the images from the accompanying video..
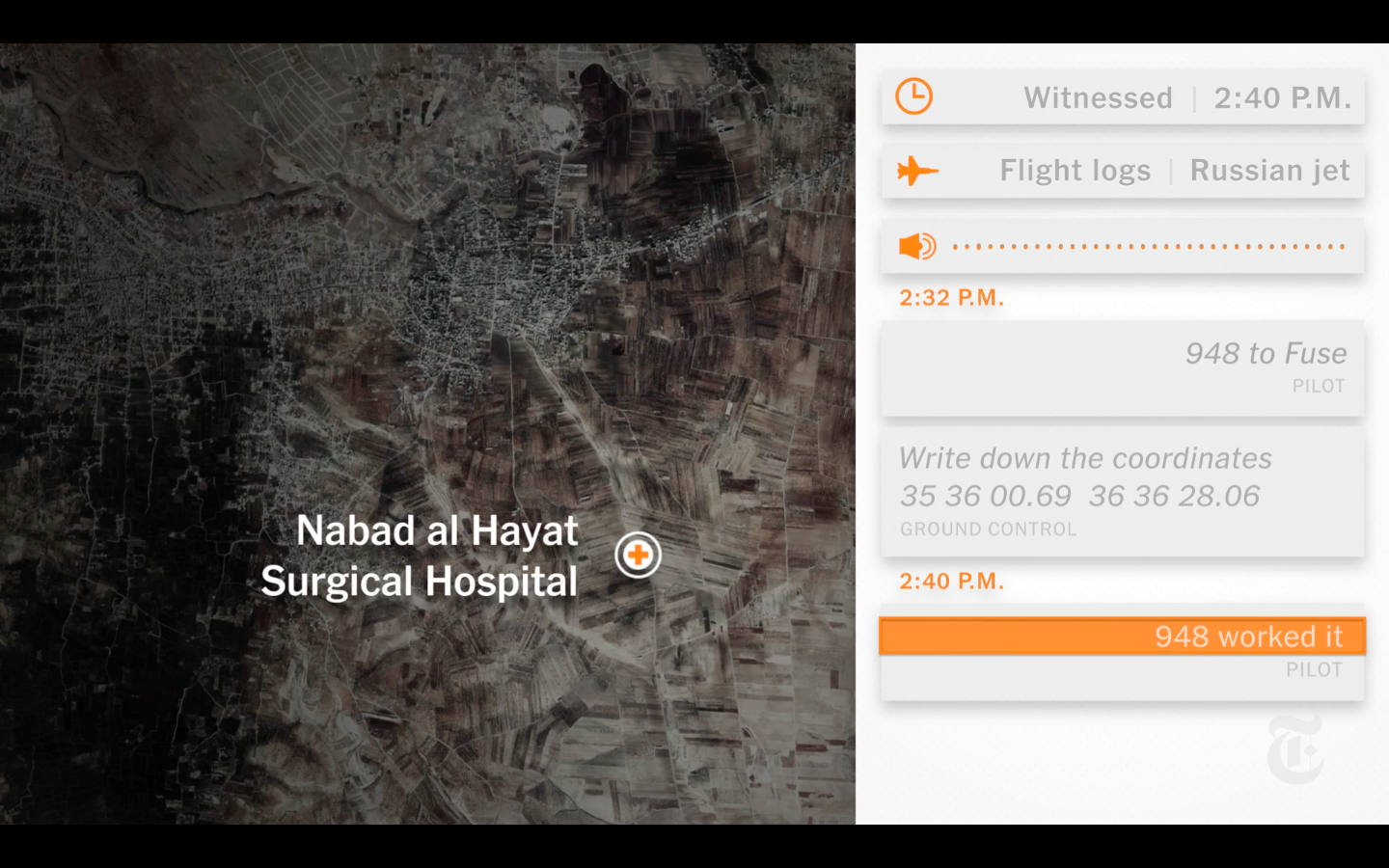
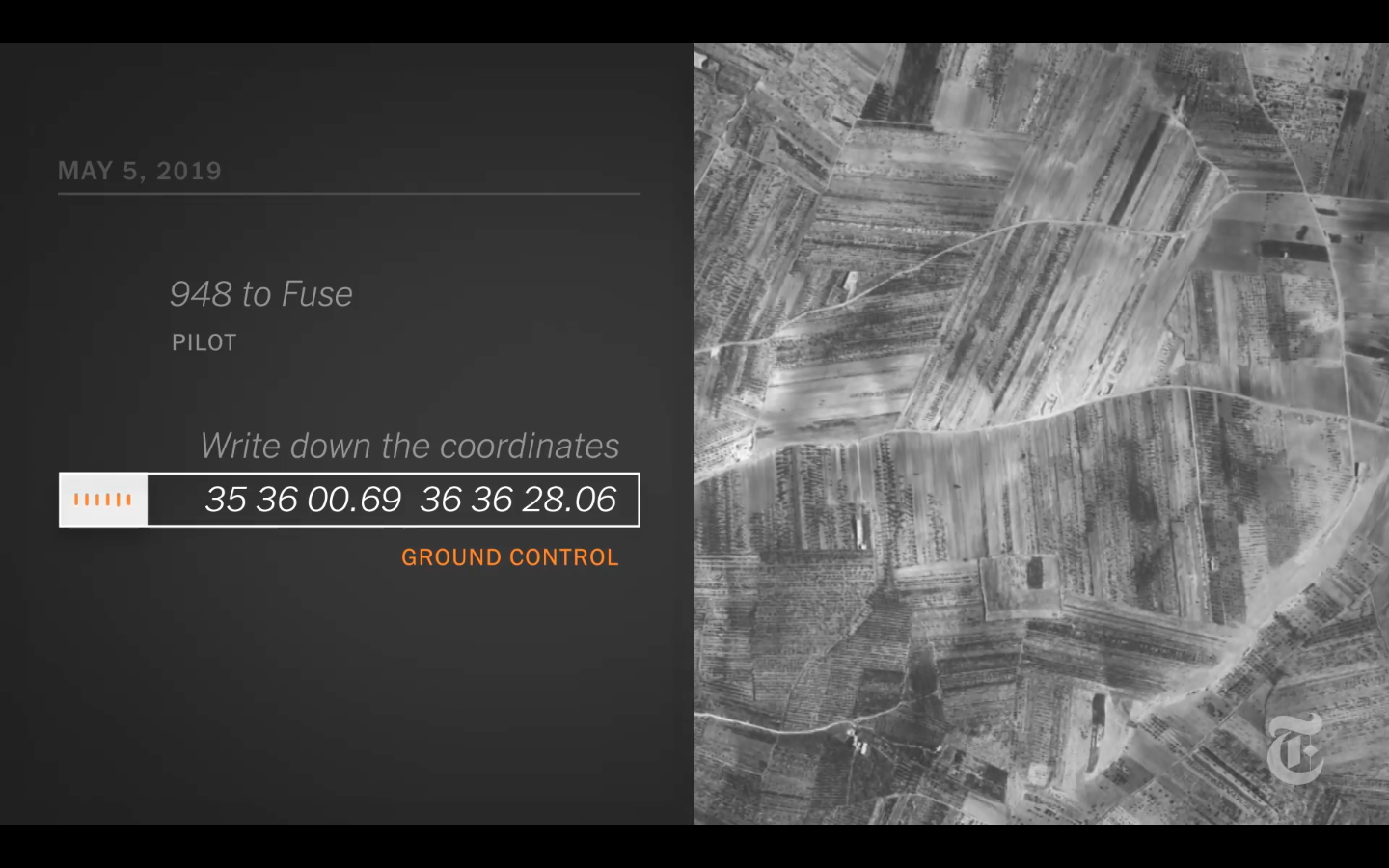
Nabad al Hayat had been attacked three times since it opened in 2013 and had recently relocated to an underground complex on agricultural land, hoping to be protected from airstrikes.
At 2:32 p.m. on May 5, a Russian ground control officer can be heard in an Air Force transmission providing a pilot with a longitude and latitude that correspond to Nabad al Hayat’s exact location.
At 2:38 p.m., the pilot reports that he can see the target and has the “correction,” code for locking the target on a screen in his cockpit. Ground control responds with the green light for the strike, saying, “Three sevens.”
At the same moment, a flight spotter on the ground logs a Russian jet circling in the area.
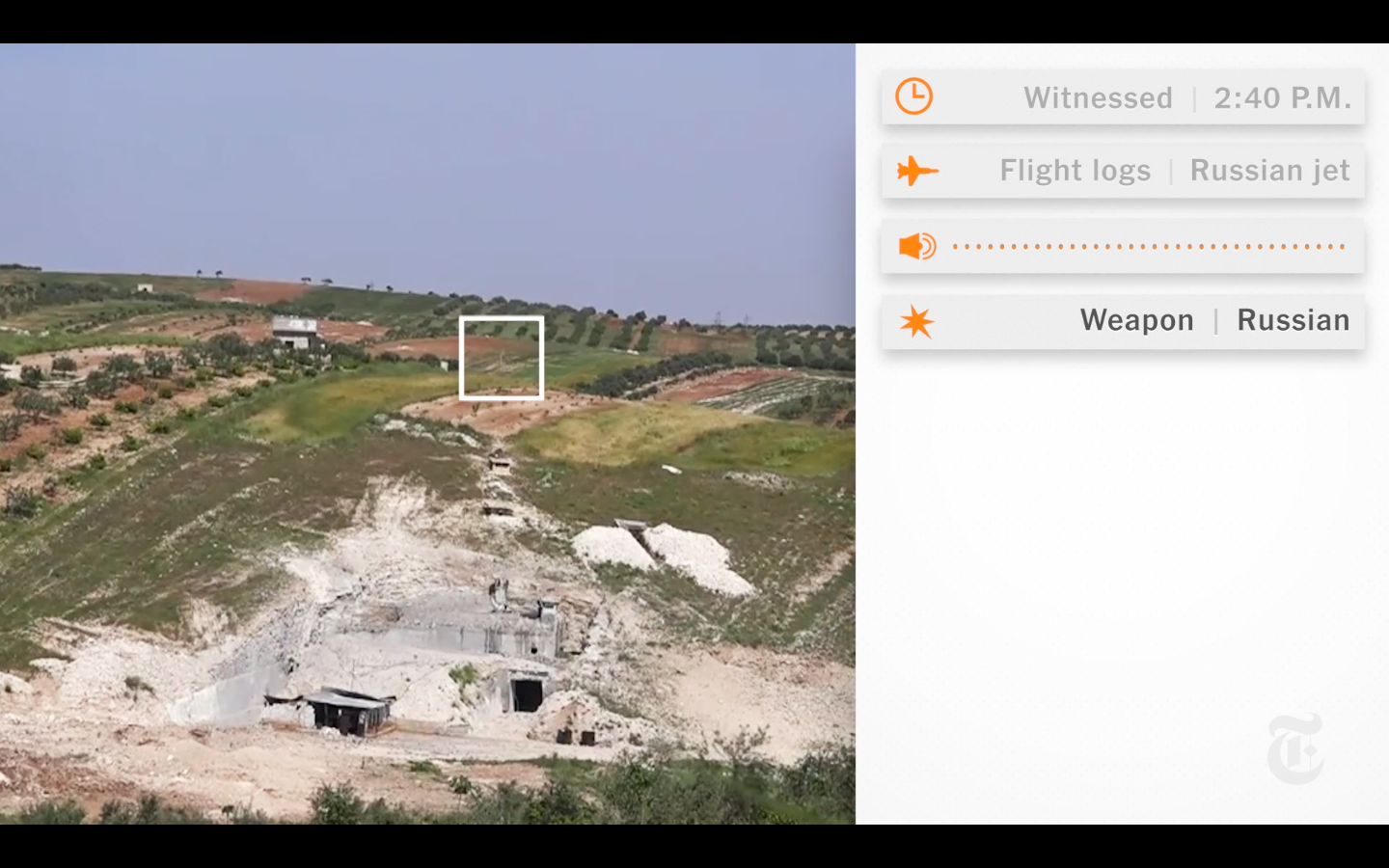
At 2:40 p.m., the same time the charity said that Nabad al Hayat was struck, the pilot confirms the release of his weapons, saying, “Worked it.” Seconds later, local journalists filming the hospital in anticipation of an attack record three precision bombs penetrating the roof of the hospital and blowing it out from the inside in geysers of dirt and concrete.
The staff of Nabad al Hayat had evacuated three days earlier after receiving warnings and anticipating a bombing [which is how journalists came to be on site to film the strike].
Another attack – detailed in the accompanying video – was on the Kafr Zita Cave Hospital (see also here).
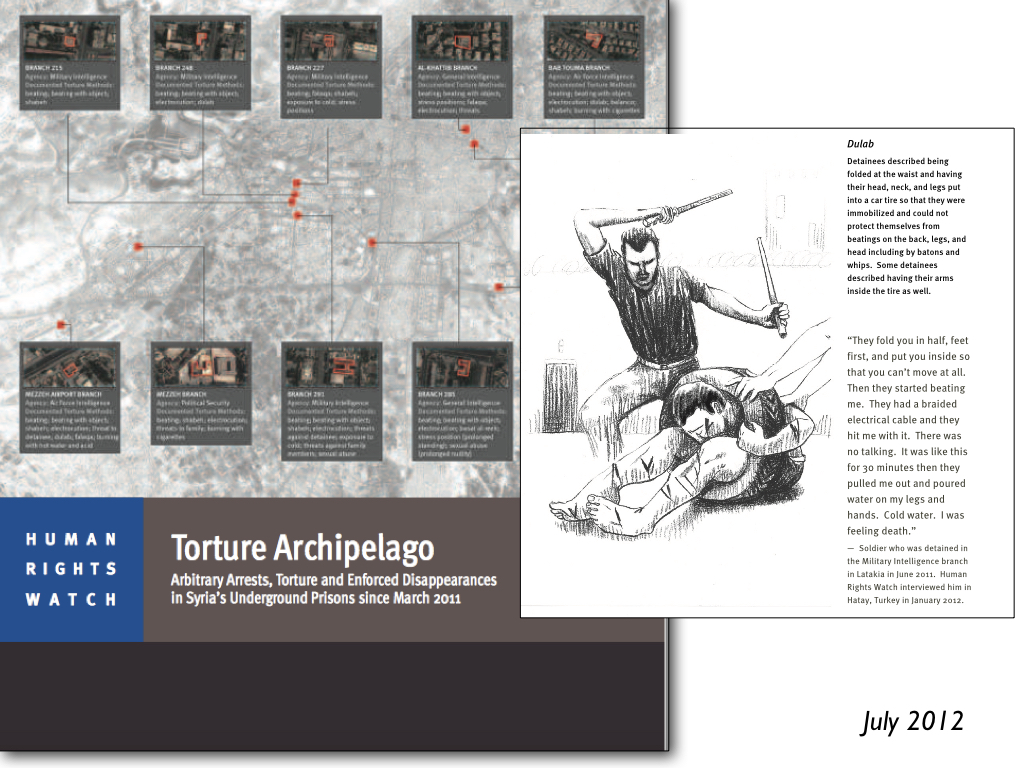
As I’ve explained elsewhere, spaces of exception are not confined to the camp (as Agamben and others claim); war zones are also spaces in which particular groups of people are knowingly and deliberately exposed to death by removing the legal protections that would ordinarily safeguard them. But these are not legal ‘black holes’ either. The removal of those protections is itself (in part) the product of legal manoeuvers and, in the case of Syria, sleight of hand: Assad’s counterterrorism laws criminalised all medical aid to the opposition. That legal armature extends beyond domestic legislation: international humanitarian law and other quasi-legal formularies (including Rules of Engagement) are supposed to afford a modicum of protection to civilians. But throughout, hospitals and clinics are supposed to be ‘exceptions to the exception’: attacks on them, their staffs and patients are explicitly proscribed under IHL.
I’m bringing all these materials together – from attacks on hospitals on the coast of France and the Western Front in the First World War through Afghanistan (here and here) and Syria – in a major new essay: more soonest, though like most of my essays these days it threatens to metamorphose into a small book….
That essay will also elaborate the claims set out in the summary image above. One of the crucial points to sharpen, I think, is that the exception often appears earlier in time and distant in space from the enclosed contours of the camp or even the war zone that has replaced the traditional ‘battlefield’. I’m thinking here (in the case of the camp in the Second World War) on the systematic denigration of the Jews, the restrictions imposed on their life and movement in occupied cities, the roundups and detentions (see my lecture on occupied Paris under the TEACHING tab), their confinement to ghettoes: all of this in advance of their brutal transportation to the death camps hundreds of miles distant. If we don’t draw attention to those preliminary steps – if we fail even to recognise them – then it will be too late: the gates of the camp will clang shut.
What has this to do with hospital attacks? Quite simply: if the preliminary de-certification of hospitals and doctors in opposition-held areas is allowed to pass unchallenged, if we fail to contest the claim that these are ‘so-called hospitals’ and ‘so-called doctors’ (a familiar tactic of the Assad regime and its apologists), if we fail to respect medical neutrality, then the exception to the exception will vanish: hospital attacks will have been normalised.
In my work on attacks on hospitals in Syria I’ve drawn attention to the remarkable Central Cave Hospital (see also here and here) – and to what it says about a war when hospitals have to be excavated deep into the ground in a desperate attempt to protect them from airstrikes.
That hospital – formally, the Al Maghara (Dr Hasan al Araj) Hospital – was excavated in the side of a mountainside at Kafr Zita in Hama and opened in October 2015. The Syrian-American Medical Society had originally proposed to build the hospital in the heart of the city, but local residents feared that doing so would turn them into targets for airstrikes.
Yet going outside and underground provided only limited protection: the hospital was repeatedly targeted by Russian and Syrian aircraft (see here and here and the videos shown by Jake Godin on Twitter here).
But as Saving Lives Underground noted (in a report co-produced with SAMS, dated May 2017), there were other cave hospitals in Syria. Compared to basement hospitals, the cave hospital is
‘a more effective protective model, in which medical facilities are built into caves carved into the side of a mountain. This model provides reasonable protective measures, but has limited feasibility as it can only be constructed in environments that contain mountains. It requires securing the entrance to the hospital, creating an emergency exit, and ensuring ventilation, but is a comparatively inexpensive model as it relies on the existing base structure of the mountain. This model has proven to be effective when designed properly and laid out with attention to details… The largest cave hospital in Syria is the Central Cave Hospital, which is 500 – 600 meters large, contains three operating rooms, and houses a range of services…’
(The most expensive model involved ‘building a new, completely underground facility. A hospital is built several meters below the surface, has a thick, reinforced concrete frame, and is covered by protective ground backfill to create the additional layer of safety. The advantage of this model is that it can be replicated anywhere with few modifications because of its standard design. However, as it involves the construction of a completely new structure, it is the most expensive model and requires the longest time to completion.’)
So there have been other cave hospitals. Now the Toronto International Film Festival features a new documentary by the co-director of the award-winning Last Men in Aleppo, writer-director Feras Fayyad, called The Cave. This was shot at another Cave Hospital in East Ghouta between 2016 and 2018 (for background, see my posts on the siege of Ghouta here and here).
Here is the Q&A with the cast and crew at TIFF:
The Cave should be shown in theatres in the fall, and (as you can see from the trailer below) is co-sponsored by National Geographic and will appear in its new documentary line-up:
The Cave follows another documentary on the work of doctors, nurses and patients under siege in Assad’s (and Putin’s) Syria, For Sama: see my notice here.
Like For Sama it too draws attention to the multiple ways in which gender and patriarchy play out in these desperate circumstances. The Cave is run by a woman, Dr Amani Ballor, and one reviewer notes: ‘When one man shows up to get medicine for his wife, he lectures the staff that women should be “at home with the family,” not running a hospital. “We voted twice,” says a male doctor on staff. “She won both times.”’
Or again, in a detailed review of the film, Eric Kohnwrites:
What makes this determined young woman tick? Speaking through a voiceover that guides the narrative along, Amani recalls growing up under “a racist and autocratic regime,” and how the war drove her to “respond to the terrible reality” through her work. At one point, a male relative of one of her patients confronts her, demanding a man be in charge. When one of Amani’s peers comes to her defense, the showdown serves as a keen snapshot of the doctor’s struggle on several fronts. Beyond encapsulating the city’s devastation, “The Cave” is an implicit critique of a war-torn society still at the mercy of antiquated values. Even in this desperate moment, her selfless acts face backlash from stern traditionalists. With nothing to lose aside from the hospital itself, Dr. Amani has no qualms about speaking her mind. “This religion is just a tool for men,” she says.
Writing in Variety, Tomris Lafflydescribes Dr Amani working with two other women, Dr Alaa and a nurse Samaher, as a vital thematic arc of the film:
In the end, it is the feminine camaraderie and understanding that stands tall as the backbone of the film and perhaps even the entire operation. Despite having their physical safety incessantly threatened — above the ground, there is nothing but a wasteland of a city nearly flattened by bombs — and capability repeatedly questioned by male patients, the trio of women somehow manages to carve out an alternative space for themselves. In that, they criticize religion as an enabler of falsely perceived male superiority and work side-by-side with male colleagues as equals, even if their parity comes as a consequence of the desperate aboveground circumstances.
Much to think about here, clearly: another of the essays on which I’m still working, converting these various posts into long form (and always, so it seems, into very long form!), recovers the genealogy and the geography of hospital attacks in modern war – from the bombing of hospitals on the Western Front in the First World War (there’s a preliminary version here, but I’ve since done much more work) right through to the US bombing of the MSF Trauma Centre in Kunduz (see here and here) and the continuing attacks on medical care in Syria. I’ll do my best to keep you posted.
I’ve been working on my essay on ‘Woundscapes of the Western Front, 1914-1918’. What follows is the section dealing with the act of being wounded, drawn from a series of diaries, letters and memoirs; it’s followed by a section fleshing out the concept of a woundscape which I’ll post in due course [for a preliminary sketch, see here].
Subsequent sections reconstruct the precarious journey of casualties from the point of injury through the aid posts, dressing stations and casualty clearing stations to the base hospitals on the French coast and beyond (for a quick sketch, see here, and for an experimental version inspired by Harry Parker‘s Anatomy of a soldier, see here).
This is very much a working version, so please read it as such – and as always I’d welcome any comments or suggestions. I’ve added some links and images (most of them from my presentations), though those included in the final version are likely to be different.
I should add that this is one part of a much larger project that also considers medical care and casualty evacuation in other war zones: the Western Desert in the Second World War, Vietnam, and Afghanistan and Syria today.
***
John Keegan once remarked that in military histories the wounded seem to ‘dematerialize as soon as they are struck down’. [1] This matters for more than historical reasons, however, because the wounded serve as a testament to what Elaine Scarryinsists is ‘the main purpose and outcome of war’, which is to say injuring. This ugly fact, she argues, can be ‘made to disappear from view along many separate paths.’ [2] In order to bring it back, I attempt to have the wounded reappear on – and through – the paths they followed after they were injured. Most of what I have to say is confined to the British Army and its colonial and imperial counterparts from Australia, Canada, India, New Zealand and South Africa on the Western Front. [3] The details differ in other militaries and other theatres, but the elemental geography of casualty evacuation was a general one. My focus is confined to the effects of physical injury and I do not directly address what was eventually diagnosed as ‘shell shock’, but it will soon become clear that the trauma of being wounded was far from a purely physical affair and that it was suffused with emotional reactions that played a vital role in rescue and recovery. [4]
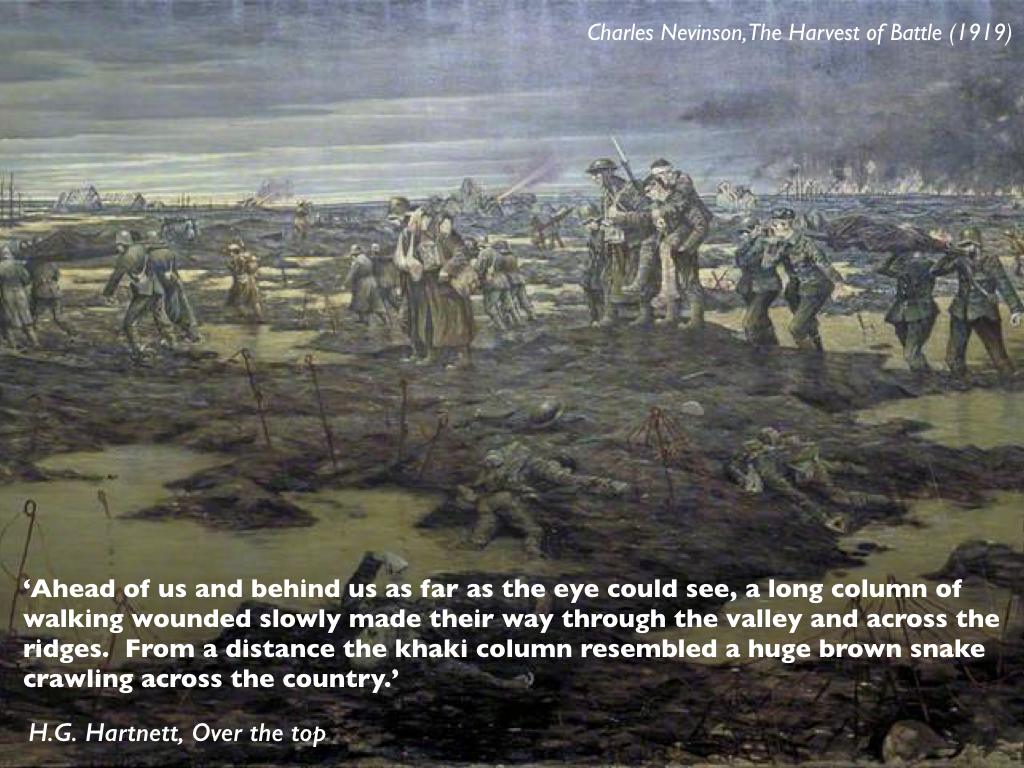
Trauma typically ruptures ordinary language – another of Scarry’s astute insights – and it is scarcely surprising that many witnesses to the broken bodies trailing across the battlefields should have turned to metaphor to convey the enormity of the toll.[5] On 1 July 1916, the first day of the battle of the Somme [above], a British officer found his trench ‘blocked with wounded men who were trying to make their way back to the dressing station’, and as Capt Radclyffe Dugmore surveyed the scene he was struck by the mechanical nature of both military violence and military medicine.
‘Here was this line of men, who little more than an hour ago were normal men in the finest of health and strength, and now maimed, and with every degree of injury, they painfully made their way back to the human repair department. The well men were rapidly moving eastward in countless numbers, going forward to the assistance of their comrades, while the injured so laboriously dragged their way back, two human streams, the sound and the unsound. Before us, all energies were devoted to destruction; behind us, all human power and skill tried to repair the damage.’ [6]
.The language of ‘wrecks’ was commonplace. To Sister Kate Luard ‘the wards [were] like battlefields, with battered wrecks in every bed.’ The task of casualty evacuation, explained one medical orderly, was ‘to move these helpless pieces of wreckage, as rapidly and comfortably as may be, to the place where they will in due course be repaired.’ [7] The language of ‘repair’ was a common one too, and I will return to its significance shortly.
Three weeks after Dugmore’s observation, and not far from his position, a wounded Australian soldier making his way from aid post to dressing station described the same awful scene but in a different, animate register:
‘Ahead of us and behind us as far as the eye could see, a long column of walking wounded slowly made their way through the valley and across the ridges. From a distance the khaki column resembled a huge brown snake crawling across the country.’ [8]
Hartnett’s pained allusion was evidently not to a serpent entwined around a staff, the classical symbol for medicine; the intended effect was altogether more venomous. [9] Still more sinister was the common imagery of the shambles and the slaughterhouse. Wilfred Owen described the infantry training camp on the French coast at Étaples as ‘neither France nor England, but a kind of paddock where the beasts are kept a few days before the shambles.’ In the sixteenth century a shambles was an open-air slaughterhouse, and the term was readily extended to the modern battlefield. Watching the stretcher-bearers file past after the Battle of Festubert with their burden of bloodied bodies one Guards officer recoiled in horror: ‘fine upstanding fellows only a few hours before’, they had become ‘nauseatingly repulsive’, ‘hideously injured carcases.’ Doctors sometimes had the same reaction and resorted to the same imagery. ‘Although but a middleman,’ confessed Capt Lawrence Gameson at a dressing station on the Somme, ‘one gets sick of blood’s smell and of the endless everlasting procession of red raw human meat passing through our hands.’If the injured survived they were consigned to a Casualty Clearing Station, what one senior medical officer – one of many, as it turns out – called his ‘Butcher’s Shop’, wherein Philip Gibbwas nauseated by the ‘great carving of human flesh’. One chaplain remembered a surgeon who had been working 24 hours without a break: ‘In the middle of it all he turned away from one table and looked up as another one was being carried in, and he shook his head. He was covered in blood – we all were – and he said, “This isn’t a hospital, it’s a butchery.”’ [10]
Those two imaginaries, the mechanical and the animate, collided most explosively and intimately in the act of being wounded. Those who wrote about it often expressed their surprise, even disbelief that it had happened to them – pain came later – or registered the immediate sensation of a tremendous blow. On the first day of the Somme it never occurred to Lt Edward Liveing that he had been wounded:
‘Suddenly I cursed. I had been scalded in the left hip. A shell, I thought, had blown up in a water-logged crump-hole and sprayed me with boiling water. Letting go of my rifle, I dropped forward full length on the ground. My hip began to smart unpleasantly, and I felt a curious warmth stealing down my left leg. I thought it was the boiling water that had scalded me. Certainly my breeches looked as if they were saturated with water. I did not know that they were saturated with blood.’ [11]
But when Sgt R.H. Tawney was hit later the same day he had no doubt he had been hurt:
‘I felt … that I had been hit by a tremendous iron hammer, swung by a giant of inconceivable strength, and then twisted with a sickening sort of wrench so that my head and back banged on the ground, and my feet struggled as though they didn’t belong to me. For a second or two my breath wouldn’t come. I thought – if that’s the right word – “This is death”, and hoped it wouldn’t take long. By-and-by, as nothing happened, it seemed I couldn’t be dying. When I felt the ground beside me, my fingers closed on the nose-cap of a shell. It was still hot, and I thought absurdly, in a muddled way, “this is what has got me”. I tried to turn on my side, but the pain, when I moved, was like a knife, and stopped me dead. There was nothing to do but lie on my back.’ [12]
Three weeks later, still on the Somme, Lt Robert Graveshad a similar sensation when he was seriously wounded. ‘An eight-inch shell burst three paces behind me,’ he recalled.
‘I heard the explosion, and felt as though I had been punched rather hard between the shoulder blades, but without any pain. I took the punch merely for the shock of the explosion; but blood trickled into my eye and, turning faint, I called to Moodie [his company commander]: “I’ve been hit.” Then I fell…’ [13]
His friend Lt Siegfried Sassoon’s reaction to being wounded during the Battle of Arras the following year)was much the same. He too knew at once that he had been hurt, even if he was not sure how. ‘No sooner had I popped my silly head out of the sap,’ he wrote much later, ‘than I felt a stupendous blow in the back between my shoulders. My first notion was that a bomb [grenade] had hit me from behind, but what had really happened was that I had been sniped from in front…To my surprise I discovered that I wasn’t dead.’ [14]
As these accounts indicate, for many wounded soldiers the proximity of death was palpable: space sensibly contracted to their wound, their body and its immediate surroundings. ‘A man badly knocked out feels as though the world had spun him off into a desert of unpeopled space,’ Tawney admitted: a feeling heightened by the standing order forbidding troops from stopping to aid the wounded during an advance. ‘Combined with pain and helplessness,’ he continued, ‘the sense of abandonment goes near to break his heart.’ [15] When Pte David Jones was shot in the leg on the Somme shortly after midnight on 11 June 1916, and left barely able to crawl, a corporal hoisted him on his back until a major saw what he was doing and told him:
‘“Drop the bugger here” for stretcher-bearers to find. If every wounded man were to be carried back, their firepower would be cut in half. “Don’t you know there’s a sod of a war on?”’ [16]
Many of the seriously wounded stumbled or crawled into shell-holes to wait for their rescuers; some lay out for days. On the first day of the Somme Pte A. Matthews was escorting German prisoners back across No Man’s Land, that narrow strip between the opposing lines of trenches, when he was shot in the thigh. An officer dragged him into a disused trench and bound up his wound as best he could before rejoining the advance. While the trench sheltered Matthews from direct fire (‘shells were bursting all around me’), he realised that unfortunately it also concealed him from the view of any rescuers. Later that day a company runner chanced to see him and left his water-bottle, but Matthews was unable to move – ‘I might as well have been chained to the ground’ – and as night fell all he could do was shout for help. Nobody came. He eked out his iron rations and water, but by the third day it was all gone. The next night a group of wounded men making their way back found Matthews, and shared the iron rations they had scavenged from the dead. They could do no more for him, but promised to get help. An hour or two later they returned, disoriented, and set off in a different direction. The next night they came back again, ‘in a terrible state’, one of them crawling on his hands and knees. They shared some biscuits and water before setting out once more; Matthews never saw them again. The next morning a shell-burst buried the biscuits and pierced his water-bottle, and he was reduced to catching rain in his helmet and drinking from pools of water in the trench. He drifted in and out of consciousness until, ten days later, an officer on patrol found him – ‘nearly treading on me’ – and dug him out before getting him onto a stretcher. When he reached the Advanced Dressing Station at Sailly he was ‘a mere skeleton’: he had been lying out in No Man’s Land for 14 days. [17] This was something of a record; Matthews’s experience combines bad luck and good luck in equal measure, and it is impossible to know how many others succumbed to their injuries while waiting or, perhaps like the party of wounded men who stumbled back to his trench time and time again, never made it to safety.
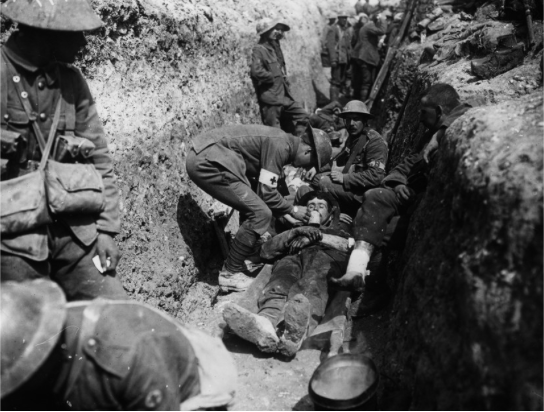
If they were fortunate the wounded would have others for comfort and company while they waited, but all any of them had for first aid was a field dressing and an ampoule of iodine. Capt Harold McGill reckoned that ‘the obsessing fear of the men was death from hemorrhage’ – understandably so in the absence of effective blood transfusion until late in the war – and the field dressing was the first vital response to bring bleeding under control. [18] One soldier explained:
‘The first field dressing which each man carries sewn in the lining of his tunic has saved many lives. Comprising as it does two pads of gauze and cotton-wool and a bandage, it can be ripped out of its case and clapped on to the wound, and so save the injured man, who may have to lie out hours before he can be taken back to a dressing-station, many risks from loss of blood or outside infection.’ [19]
Of course, the utility of the dressing depended on the nature of the wound. The same man recalled a lecture from his Medical Officer, who had explained that a field dressing could be used to stop bleeding from an arm or a leg, but ‘if the man was hit in the body or head – well, the doctor shrugged his shoulders in a way that made us think.’ [20]If they were not alone the wounded might also be able to improvise a tourniquet or even a splint with their bayonet or rifle, and if the iodine bottle had not smashed – unlikely, McGill thought: ‘The men reported to me that during the action they had nearly always found their pocket ampoules of iodine tincture broken when the time came to use them’ [21]– they could make a rudimentary attempt at cleaning the wound.
Given the cascading combination of immediacy, difficulty and uncertainty it is scarcely surprising that the space of the wounded should have contracted so drastically. And yet at the same time that space expanded, partly through what had become the taxing task of traversing even a short distance to relative safety, and partly through the tantalizing prospect of a ‘Blighty’, a wound judged sufficiently serious to require evacuation to Britain (and perhaps beyond for troops who came from elsewhere in the Empire). [22]
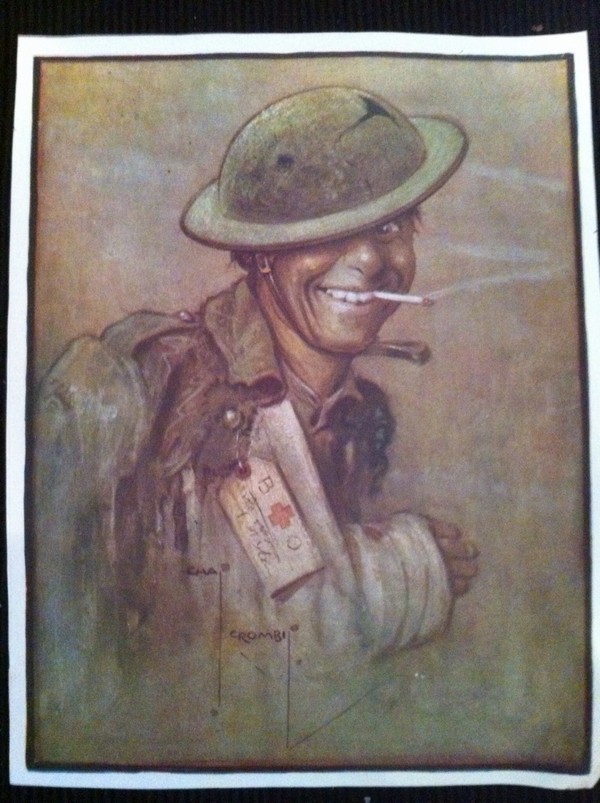
Arthur Empey came round from surgery at a Casualty Clearing Station to find rows of soldiers lying on stretchers: ‘The main topic of their conversation was Blighty. Nearly all had a grin on their faces.’ [23] One medical orderly explained that ‘a wound, even when serious, is the messenger of freedom’ – and he had never met a wounded man who wanted to return to the trenches. [24]Another had ‘only heard of one who said that he was anxious to return there, and he was subsequently transferred to No. 2 General Hospital in Le Havre, where the huge numbers of mental cases were cared for.’ [25]
Even so, the extended space of evacuation was a fraught and dangerous one. Many of the wounded fell in No Man’s Land, in the front-line trenches themselves, or in broken land during the fluctuating tides of advance and retreat in the opening and closing phases of the war. They were injured in major offensives (‘pushes’), in small raids (‘stunts’) and by routine, almost ritualized shelling and firing (‘the morning hate’). These were the most immediate danger zones in space and in time, extending back towards the reserve trenches and the small towns and villages in the rear. The wounded were supposed to move within a legal envelope that protected them from further attack. The Hague Regulations stipulated that ‘all necessary steps must be taken to spare’ – as far as possible – ‘places where the sick and wounded are collected.’ But that possibility was none the less limited. Firing and shelling were often notoriously inaccurate, casualty clearing stations were routinely located close to batteries and railheads, and it was not always easy to make out the red cross symbol that was supposed to guarantee protection. In the final months of the war even base hospitals on the French coast were bombed, while hospital ships crossing the Channel ran the gauntlet of mines and torpedoes. [26] If the wounded imagined travelling through an extended space towards safety, then it was a safety rendered conditional by the continued risk of attack. And the journey itself always exacted its own, sometimes deadly toll on the wounded body, which prompted Patrick MacGillto write of being ‘a passenger on the Highway of Pain that stretched from Lens to Victoria Station’. [27]
My purpose is to reconstruct that highway and the relationship between wounded bodies and the journeys they undertook. Many of those planning for war had a remarkably sanitized view of both. When one hard-pressed volunteer with the British Red Cross Society, working at a field hospital in Belgium in September 1914, described her pre-war training she recalled
‘the drill and the white-capped stretcher-bearers at home, and the little messenger boys with their innocuous wounds, which were so neatly and laboriously dressed.
The messenger boys’ wounds were always conveniently placed, and they never screamed and writhed or prayed for morphia when they were being bandaged. And shoulders were not shot away, nor eyes blinded, nor men’s faces – well, not much good ever came of talking of the things one has seen, and they are best left undescribed. “These are not wounds, they are mush,” I heard one surgeon say; and then I thought of the little messenger boys and their convenient fractures.’ [28]
The wounds were not the stylised, artfully coloured images of the text book and when G.H. Makins suggested that a survey of them ‘forcibly reminds the observer of the water-colour drawings made by Sir Charles Bell’ he was referring to Bell’s extraordinary ability to convey the horrific damage wrought by musket balls and shrapnel during the Peninsular War. Bell was a military surgeon and his sketches were no less remarkable for their rendering of the agony, despair and sheer terror of the wounded: a far cry, as he noted, from the text-books. [29]
Similarly, schemes for medical evacuation typically displayed an elegant linear geometry, an abstract grid of transmission lines that resembled what Fiona Reidcalled ‘a modernist dream’ with no catastrophic breaks or nightmare tangles (Figure 3). [30] This highly imaginative geography of an evacuation machine, carefully oiled and smoothly running, intersected with debates around a politics of speed. [31] [For much more, and a detailed case study, see my post on ‘The Leaden Hours’ here]. In the first months of the war there were complaints that it was taking far too long for the wounded to be brought from the firing zone to hospitals on the French coast. These reports provoked sufficient public unease for Lord Kitchener, Secretary of State for War, to send Col Arthur Lee to France to investigate. In a series of private communications Lee conceded that ‘in surveying the scene from London, or studying it upon a map, questions of transport present no very serious difficulties’, whereas once in France it quickly became obvious that getting the wounded to railheads was complicated by intense enemy shelling, and that the railways were under enormous pressure – ‘the wounded must of course give way to food, ammunition and reinforcements for the fighting forces’ – and with many bridges destroyed and signalling systems dislocated the hastily improvised ambulance trains, often little more than cattle trucks filled with straw, had ‘to slowly explore their own way back towards [the hospitals at] the Base.’ [32] Two years later the politics of speed had reversed; the concern now was that the RAMC had become so fixated on rapid evacuation that the injured were suffering needlessly. The debate reached its climax when Sir Almroth Wright, Consultant Physician to the British Expeditionary Force, criticized what he saw as the preoccupation with rapid evacuation, ‘hustling the wounded from hospital to hospital’ he called it, and the overwhelming importance attached to ‘the fact that a [Casualty Clearing Station] has passed so many thousands or tens of thousands of wounded through the wards, evacuating these in a minimum of time so as to be at disposal for reception of more patients.’ He claimed that as soon as a new convoy arrived at a base hospital, and as a direct result of ‘the catastrophes which are associated with long journeys’ from the Casualty Clearing Station, ‘amputations and other operations in large numbers have to be performed upon men who had been judged fit to travel’ (my emphasis). Wright’s complaints were summarily – and angrily – dismissed as ignorant and even ‘stupid’ in what was a bitter personal dispute, and the official response doubled down on the machine-like efficiency of the evacuation system.
What flickers in the fissures of these exchanges is the stubbornly, viscerally bio-physical: injured bodies did not present themselves as pristine plates in a medical atlas and their precarious journeys were not inscribed on the paper trails of an evacuation plan. The relations between the two were not only intimate; they were also reciprocal. The nature of the wound materially affected evacuation. Treatment times and pathways for ‘walking wounded’ and stretcher-cases were different, for example, and the worst cases were often the last to reach a Casualty Clearing Station and – if they survived – they travelled much further down the line and ultimately back to Britain. Those journeys in turn affected the wound: rescuing casualties from No Man’s Land was almost always at the risk of further injuries from enemy fire, for example, and as bearers struggled to carry stretchers over shell-shattered ground and through waterlogged trenches, as ambulances bumped and skidded over muddy tracks and torn-up roads, and as ambulance trains clanked and wheezed their way to the coast, the spasmodic jolting greatly aggravated pain and increased the risk of haemorrhage.
To be continued
[1]John Keegan, The Face of Battle(London: Pimlico, 2004), p. 40; Keegan was referring specifically to General Sir William Napier’s account of the battle of Albuera in 1811, but he was also sharpening a general point.
[2]Elaine Scarry, The Body in Pain: the making and unmaking of the world (New York: Oxford University Press, 1985) p. 64.
[3]Regiments were raised from other British colonies in the Caribbean and Africa too, and also in Newfoundland; in some cases colonial and imperial casualties were treated by their own medical services, and in others by the RAMC, though they all worked in close concert with one another. For a general discussion, which extends to the French and German medical services, see Leo van Bergen, Before my helplesssSight: suffering, dying and military medicine on the Western Front, 1914–1918 (London: Routledge, 2016).
[4]On ‘shell shock’ and, of direct relevance to my discussion, what was known as ‘wound shock’, see Stefanos Geroulanos and Todd Myers, The human body in the age of catastrophe: brittleness, integration, science and the Great War(Chicago: University of Chicago Press, 2018) especially Ch. 2.
[5]Casualty estimates are notoriously difficult, but on the Western Front more than five million from the Allied armies were wounded, most of them from France and the United Kingdom, and more than three million from the Central Powers, principally Germany and Austria-Hungary. There were also tens of thousands of civilian casualties, from towns and villages close to the front lines but also from long-distance shelling and air strikes much more distant from battlefields whose boundaries were already dissolving.
[6]Captain A. Radclyffe Dugmore, When the Somme ran red(New York: George H. Doran, 1918) pp. 201-2. Hence too Mark Harrison’s apt description of a ‘medical machine’ assembled on the Western Front: The Medical War: British Military medicine in the First World War (Oxford: Oxford University Press, 2010). The imagery of two streams was a common one too, and so was its mechanical rendering. ‘One of the most stabbing things in this war,’ wrote Sister Kate Luard, ‘is seeing the lines of empty motor ambulances going up to bring down the wrecks who at this moment are sound and fit, and absolutely ready to be turned into wrecks’: John Stevens (ed) Unknown warriors: the letters of Kate Luard1914-1918(Stroud, UK: History Press, 2014) 8 May 1915.
[7]Stevens, Unknown warriors, 10 April 1917; Ward Muir, ‘An intake of wounded’, in Happy though wounded: the book of the 3rdLondon General Hospital(London: Country Life, 1917) p. 64.
[8]H.G. Hartnett, Over the top(Sydney: Allen and Unwin, 2009) p. 60; Hartnett wrote his memoir in the early 1920s from diaries he had kept during the war.
[9]His own journey was a long and painful one. ‘After tramping five or six miles in search of medical attention,’ Hartnett continued, he and his mates ‘finally reached Albert, where the confusion was even worse if that was possible. Long lines of wounded men along the footpaths and roadways were waiting their turn to get attention from doctors and their assistants, stationed at intervals along the roads, out in the open’ (p. 61). From Albert he was taken by lorry and light railway to a casualty clearing station and, after his wound had been dressed, by ambulance train to Rouen; then it was on to Le Havre and a hospital ship bound for Southampton.
[10]Wilfred Owen, Collected Letters(ed. Harold Owen and John Bell) (Oxford: Oxford University Press, 1967) 31 December 1917; ‘An O.E.’ [G.P.A. Fildes], Iron times with the Guards(London: John Murray, 1918) pp. 74-5; Lawrence Gameson, Private Papers, IWM Doc 612; Philip Gibbs, Now it can be told(New York: Harper, 1920) p. 374; Capt Leonard Pearson, in Lyn MacDonald, The Roses of No Man’s Land(London: Penguin, 1993) p. 187.
[11]Edward G.D. Living, Attack: An Infantry Subaltern’s Impression of July 1st, 1916 (New York: Macmillan, 1918) pp. 69-70. He managed to walk out after one of his men applied iodine and a field dressing to his wound, but walking became steadily more painful; eventually, weak from loss of blood, he was placed on a stretcher and wheeled to an advanced dressing station, and from there he was taken by ambulance to a Casualty Clearing Station.
[12]R.H. Tawney, ‘The attack’, Westminster Gazette, 24-5 October 1916.
[13]Graves confessed that his memory of what happened next was ‘vague’. He was not expected to survive, and was taken to a dressing station where he remained unconscious; when his commanding officer went down and saw him lying in a corner ‘they told him I was done for.’But the next morning an ambulance took Graves to a Casualty Clearing Station, where he remained until 24 July when he was put on an ambulance train for a Base Hospital on the coast and was eventually repatriated to Britain. Meanwhile his commanding officer had written to his mother tendering his condolences at the loss of her son. Robert Graves, Goodbye to all that(London: Penguin, 2000; first published in 1929) pp. 180-2.
[14]Siegfried Sassoon, Memoirs of an infantry officer(London: Faber, 1930). This is a fictionalised account of Sassoon’s experience on 16 April 1917; he recorded his more immediate reactions in his journal but said virtually nothing about the initial shock of being hit. He left the trench as ‘walking wounded’ and, after his wound was dressed at an aid post, was driven to a Casualty Clearing Station: Sassoon Journal, Cambridge University Library MS Add. 9852/1/10.h
[15]Tawney, ‘Attack’.
[16] Jones resumed his crawl and was eventually found by a bearer party: Thomas Dilworth, David Jones and the Great War (London: Enitharmon Press, 2012) p. 117. Tiplady, Soul of the soldier, p. 131 explained the logic behind the injunction: ‘When a man falls his neighbor cannot stay with him. He must press on to the objective, otherwise, if the unwounded stayed to succor the wounded, there would be none to continue the attack.’ This was of course emotionally hard. ‘The grimmest order to me was that no fighting soldier was to stop to help the wounded,’ one sergeant confessed. ‘The CO was very emphatic about this. It seemed such a heartless order to come from our CO who was … looked upon as a religious man. I thought bringing in the wounded was the way Victoria Crosses were won. But I realized that this would be an order to the CO as well as us from the General and that the whole of the attack could be held up if there were many wounded and we stopped to help them’: Sgt Charles Moss, in Richard van Emden, The Somme(Barnsley UK: Pen and Sword, 2016) p. 00.
[17]A. Matthews, ‘I was fourteen days in No Man’s Land’, I Was There!pp. 688-691; Capt A.W. French, War Diary (Liddle Collection), 14 July 1916. For another vivid account of a survivor, see the memoir written after the war by John Stafford describing his wounding on the Somme on 8 August 1916:https://www.europeana.eu/portal/en/record/2020601/contributions_3155.html?q=%22John+Stafford%22.
[18]McGill, Medicine and Duty, pp. 118-9.
[19]Arthur Mills, Hospital Days(London: T. Fisher Unwin, 1916) p. 14.
[20]Mills, Hospital days, p.
[21]McGill, Medicine and Duty, p. 157.
[22]‘Blighty’, a corruption of the Urdu vilayati(‘foreign’ or ‘European’) was first used by Indian soldiers to refer to Britain in the Boer War; its use became widespread in the First World War.
[23]Arthur Empey, Over the top(New York: G.P. Putnam, 1917) p. 00.
[24]Christopher Arnander (ed), Private Lord Crawford’s Great War Diaries(Barnsley, UK: Pen and Sword, 2013) 30 September 1915. ‘To these men,’ Crawford added, ‘the relief of leaving the front honourably wounded is inconceivable after months of killing, anxiety and fatigue.’ David Lindsay, the Earl of Crawford, enlisted in the RAMC as a private in April 1915 at the age of 43; in July 1916 he returned to the UK as a member of the coalition government.
[25]M.R. Werner, Orderly!(New York: Jonathan Cape & Harrison Smith, 1930) p. 76.
[26]Stephen McGreal, The war on hospital ships, 1914-1918(Barnsley UK: Pen and Sword, 2009).
[27]Patrick MacGill, The Great Push: an episode of the Great War(New York: Grosset and Dunlap, 1916) p. 254. This was a memoir lightly disguised as fiction; MacGill was wounded at Loos on 28 September 1915, and in the preface wrote that he had ‘tried to give, as far as I am allowed, an account of an attack in which I took part’ (p. 7).
[28]Sarah Macnaughtan, A woman’s diary of the war(London: Nelson, 1916) p. 23. Similar make-believe drills took place behind the front lines, where they were met with a healthy cynicism by ‘wounded’ and stretcher bearers alike. ‘After heavy losses we would get reinforcements and this would be followed by a Field Day to break in the newcomers’, explained one orderly with a Field Ambulance. ‘Men with labels describing their supposed injuries were hidden in unlikely spots and had to be found and dealt with as if actually wounded’: Edwin Ware, Diary,p. 94 [WL:RAMC/PE/1/707]. One private recalled a rehearsal for a ‘special stunt’ in which he played a casualty: ‘My wounds were not too painful to prevent my enjoyment of the spectacle while waiting for the stretcher bearers, who did not seem in a great hurry. Casualties here had their own choice of wounds, and they all seemed to prefer some wound which made it impossible to walk a step, much to the disgust of the stretcher bearers.After some argument with the stretcher bearers who came at last to attend to me, I was bundled unceremoniously on to a stretcher with my mess tin making itself unpleasant in the middle of my back, despite the fact that both my legs had been shattered (in theory)’: Doreen Priddey (ed.), A Tommy at Ypres: Walter’s War(Stroud: Amberley Publishing, 2011) 5-9 December 1916.
[29]G.H. Makins, ‘A note upon the wounds of the present campaign’, The Lancet, 10 October 1914 (p. 905); M.K. H. Crump and P. Starling, A surgical artist at war: the paintings and sketches of Sir Charles Bell 1807-1815 (Edinburgh: Royal College of Surgeons, 2005). Bell uncannily prefigured the horrors for which his successors were equally ill-prepared one hundred years later. ‘The cases I have had under my care,’ he wrote in his Dissertation on gunshot wounds(1814), ‘have proved to me that the books we possess upon the subject of field-practice do not even hint at the nature of the difficulties the surgeon has to encounter there.’
[30]Fiona Reid, Medicine in First World War Europe: Soldiers, Medics, Pacifists (London: Bloomsbury, 2017) p. 19.
[31]Derek Gregory, ‘The politics of speed and casualty evacuation on the Western Front, 1914-1918’, forthcoming.
Apologies for the long silence – I’ve made several trips to the UK to deliver lectures, but I’ve also been (almost literally) in the trenches. My supposed-to-be 8,000 word essay on ‘Woundscapes of the Western Front’ has morphed into a monster: 35,000 words and I’m still not done…. More on that eventually (I so hope…). But en route, and in part as a response to a question I was asked after one of my presentations, I want to elaborate on a footnote.
My essay is about the evacuation of wounded soldiers, but human bodies were not the only ones requiring medical attention on the Western Front. By August 1917 the British Army had 368,000 horses and 82,000 mules in Belgium and France. At the outbreak of the war the cavalry were expected to play their traditional role –
[Image: National Library of Scotland]
– but by the end of the war most horses were pulling gun limbers, ammunition trains, supply waggons and ambulances [more here].
Horse-drawn ambulances were never made obsolete by motor ambulance convoys. Their capacity was limited and they were very slow – ‘hopelessly immobile’, according to one senior RAMC officer – but they remained the only option in some places. On the Somme in July 1916 the ground was so pitted with shell-holes that motor ambulances could not be used close to the line and horse ambulances worked for 24 hours or more at a stretch, ferrying casualties to motor ambulance convoys waiting further back:
Not surprisingly, horses (and mules) were highly vulnerable to shelling and shrapnel, to gas attacks and, wherever environmental conditions deteriorated, to injuries from traversing near-impossible terrain:
There is a haunting scene in Erich Maria Remarque‘s All quiet on the Western Front:
‘The cries continued. It is not men, they could not cry so terribly. “Wounded horses,” says Kat. It’s unendurable. It is the moaning of the world, it is the martyred creation, wild with anguish, filled with terror, and groaning….
They’ve got to get the wounded men out first,’ says Kat. We stand up and try to see where they are. If we can actually see the animals, it will be easier to cope with. Meyer has some field glasses with him. We can make some bigger things, black mounds that are moving. Those are the wounded horses. But not all of them. Some gallop off a little way, collapse, and then run on again. The belly of one of the horses has been ripped open and its guts are trailing out. It gets its feet caught up in them and falls, but it gets to its feet again. Detering raises his ri e and takes aim. Kat knocks the barrel upwards. ‘Are you crazy?’ Detering shudders and throws his gun on the ground. We sit down and press our hands over our ears. But the terrible crying and groaning and howling still gets through, it penetrates everything. We can all stand a lot, but this brings us out in a cold sweat. You want to get up and run away, anywhere just so as not to hear that screaming any more. And it isn’t men, just horses.
Yet far more equine losses were attributed to disease than enemy action, in contrast to troop losses (the First World War was the first in which deaths from wounds exceeded deaths from disease by a ratio of 2:1). One driver had a simple explanation. ‘Owing to the importance of the horses, whose lives were of greater value than those of the men, the horse-lines were usually in places free, or practically free from “strafing”’: Charles Bassett, Horses were more valuable than men (London: PublishNation, 2014) p. 65.
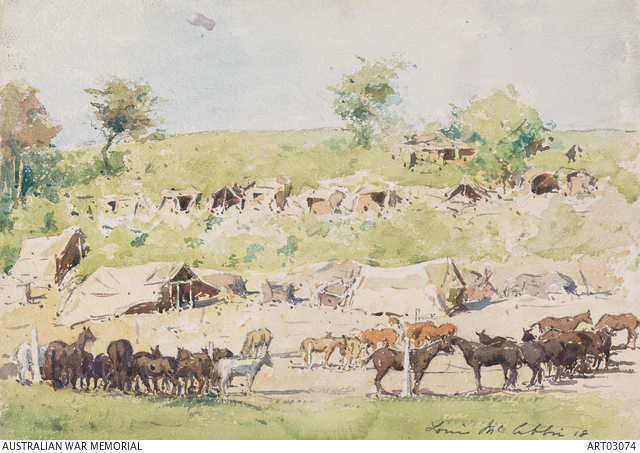
The horse-lines were indeed in the rear (see the remarkably pastoral image below: Glisy, on the Somme), but the nature of their work ensured that horses and mules had to be taken right up to the fire zone; between 1914 and 1916 battle losses accounted for 25 per cent of equine deaths, and they soared thereafter.
Last year Philip Hoaredescribed these animals as ‘the truly forgotten dead.’ He continued: ‘Sixteen million animals “served” in the first world war – and the RSPCA estimates that 484,143 horses, mules, camels and bullocks were killed in British service between 1914 and 1918.
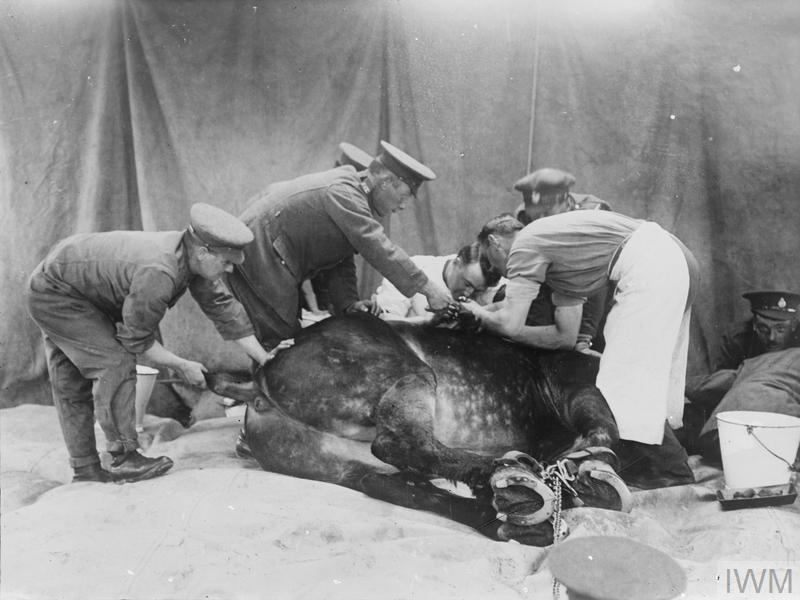
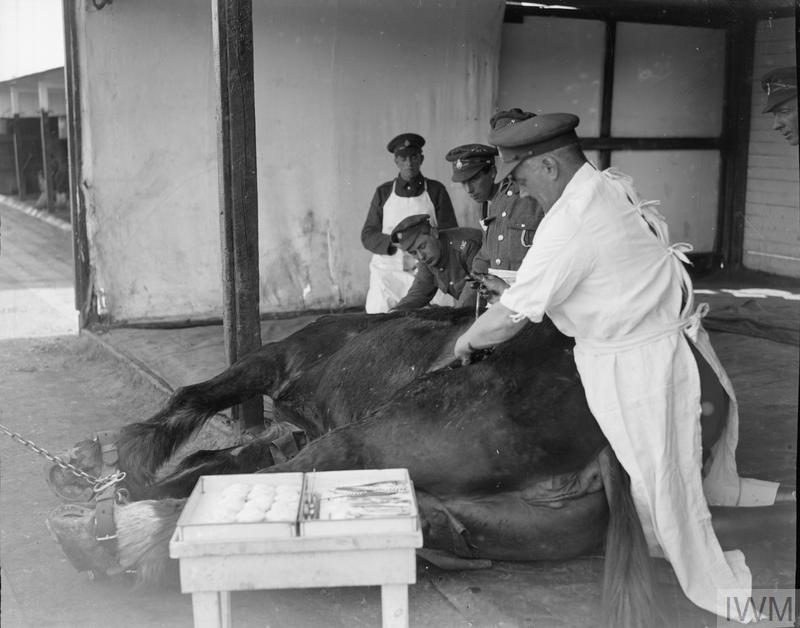
Yet, just as with human bodies, the toll of the equine dead overlooks that of the wounded. In response to the military importance of horses and mules, the (Royal) Army Veterinary Corps [the ‘Royal’ prefix was granted immediately after the war] established a system of veterinary medicine parallel to the casualty evacuation system of the Royal Army Medical Corps.
The equivalent of the Field Ambulance was the Mobile Veterinary Section; animals needing more extensive emergency care were transferred to Veterinary Evacuation Stations (the equivalent of the Casualty Clearing Station) located at railheads. They were moved either by horse-drawn ambulance –
– or by special motor ambulances designed to carry two horses each (there were 26 of them, donated by the RSPCA and subscribed from public donations):
Like wounded soldiers, horses needing further medical or surgical attention were transported by barge (mainly in Flanders: each barge could carry 32 animals) –
– or by rail to Veterinary Hospitals at the base on the French coast.
In the first months of the war cattle trucks on supply trains returning empty to the base were used (here too the parallels with the evacuation of wounded soldiers are exact!) but once the Veterinary Evacuating Stations had been established special horse trains were introduced. These had to be more or less self-sufficient: supplies of water were especially vital. Major-General Sir John Moore emphasised: ‘In transporting sick and enfeebled animals, particularly by train, which during hot seasons of the year is very exhausting, the greatest care must be exercised in watering and feeding en route.’ The need was compounded by the slow and often circuitous journeys made by trains that – like the ambulance trains carrying wounded soldiers – always had to yield to troop trains and supply trains rushing up to the front.
Between 18 August 1914 and 23 January 1919 over half a million sick and wounded animals passed through the British Army’s Mobile Veterinary Sections and Veterinary Evacuating Stations in Flanders and France. On average a special train carrying 100 sick or injured horses would arrive twice a day at each Veterinary Hospital; between 2,500 and 3,500 horses were admitted to hospital each week, and at their peak more than 4,500 were being cared for at any one time.
The capacity of these hospitals was originally set at 1,000 animals, but this was subsequently doubled. It was not uncommon, Moore explained, ‘to see three animals in the operating theatre under chloroform at the same time.’
Very few animals were allowed to stay more than three months at the base, where the hospitals operated in conjunction with Convalescent Horse Depots.
According to Moore, the core principle of the Army Veterinary Corps was ‘to get down from the front as many animals as it was possible to save; in other words to give every animal a chance.’ But what lay behind this was the same instrumentalism that guided the RAMC’s casualty evacuation model and its system of triage: the need identify the casualties most likely to survive in short order and to treat them expeditiously so that they could be returned to the front and the fight.
***
You can find more from these sources:
Simon Butler, The war horses (Halsgrove, 2011);
Stephen Corvi, ‘Men of Mercy: the evolution of the Royal Army Veterinary Corps and the soldier-horse bond during the Great War,’ Journal of the Society for Army Historical Research 76 (308) (1998) 272-84;
M-G Sir John Moore, Army Veterinary Service in War (London: Brown, 1921) [available here]
Rachael Passmore, ‘The care, development and importance of the British horse on the Western Front in World War I,’ MA thesis, Department of History, University of Leeds, 2009 [accessible here];
John Singleton, ‘Britain’s military use of horses 1914-1918’, Past & Present 139 (1993) 178-203.
Like my original essay, this post is confined to the British Army; for a remarkably detailed and beautifully illustrated account of the veterinary medical system of the US Army on the Western Front see here.
Unless otherwise credited, ALL IMAGES are Copyright Imperial War Museum, London
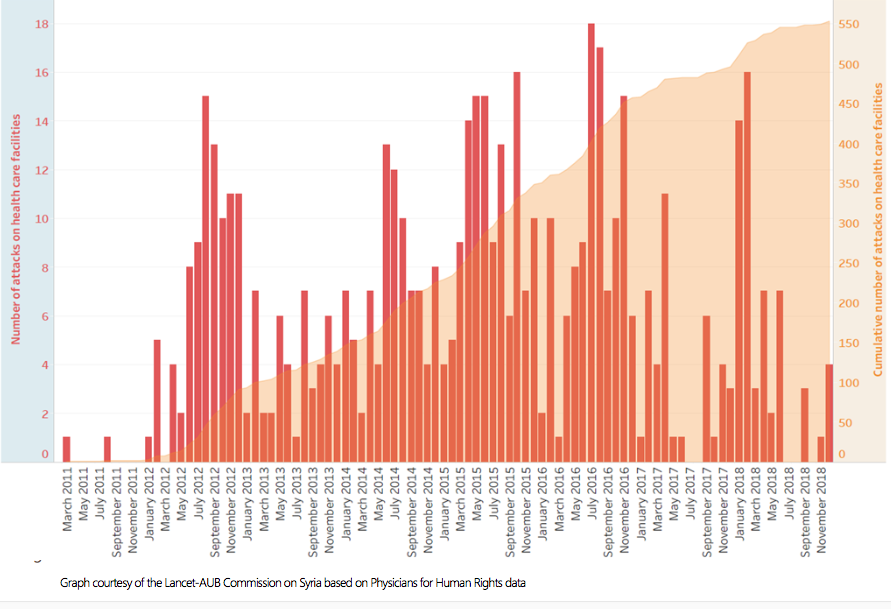
For an update and succinct review of attacks on hospitals and medical facilities in Syria – see also my ‘Your turn, doctor’ here – I recommend the latest fact-sheet from Physicians for Human Rights:
Attacks on health care, in gross violation of humanitarian norms and the Geneva Conventions, have been a distinctive feature of the conflict in Syria since its inception. PHR has documented and mapped 553 attacks on at least 348 separate facilities from March 2011 through December 2018. The reduction in the number of attacks over the past year is a clear reflection of the diminishing intensity of the conflict, which came as a direct result of the Syrian government’s takeover of most opposition-held areas. The systematic targeting of health facilities has been a crucial component of a wider strategy of war employed by the Syrian government and its allies – who are responsible for over 90 percent of attacks – to punish civilians residing in opposition- held territories, destroy their ability to survive, and draw them into government-held areas or drive them out of the country. This strategy of unbridled violence – which in addition to attacks on healthcare has included chemical strikes, sieges, and indiscriminate bombing of predominantly civilian areas – has devastated the civilian population, weakened opposition groups, and translated into direct military gains for the Syrian government.
Of the total number of documented attacks on health facilities, nearly 73 percent were carried out from the air. Nearly 98 percent of attacks on health facilities perpetrated from the air are attributable to the Syrian government and its ally Russian, which entered the conflict in 2015.
The share of attacks on health facilities from the air has grown from 38 percent of the total in 2012 to 90 percent in 2018. The Syrian government became steadily more reliant on airpower as the conflict evolved. Through their air forces, the Syrian government and Russia extended their strategy of collective punishment deep into opposition-held territory and far beyond hardened front lines. The Syrian government and its allies disabled or destroyed hundreds of facilities through aerial bombardment, leaving countless civilians without access to vital medical services.
The latest 20-page report from the Independent International Commission of Inquiry on the Syrian Arab Republic to the UN’s Human Rights Council is here. I’ve drawn on many of these reports for my continuing work on siege warfare in Syria (see for example here, here and here), and this report – based on investigations carried out from 11 July 2018 to 10 January 2019 – makes for grim reading. Here is the summary (but you really need to consult the full report):
Extensive military gains made by pro-government forces throughout the first half of 2018, coupled with an agreement between Turkey and the Russian Federation to establish a demilitarized zone in the north-west, led to a significant decrease in armed conflict in the Syrian Arab Republic in the period from mid July 2018 to mid January 2019. Hostilities elsewhere, however, remain ongoing. Attacks by pro-government forces in Idlib and western Aleppo Governorates, and those carried out by the Syrian Democratic Forces and the international coalition in Dayr al-Zawr Governorate, continue to cause scores of civilian casualties.
In the aftermath of bombardments, civilians countrywide suffered the effects of a general absence of the rule of law. Numerous civilians were detained arbitrarily or abducted by members of armed groups and criminal gangs and held hostage for ransom in their strongholds in Idlib and northern Aleppo. Similarly, with the conclusion of Operation Olive Branch by Turkey in March 2018, arbitrary arrests and detentions became pervasive throughout Afrin District (Aleppo).
In areas recently retaken by pro-government forces, including eastern Ghouta (Rif Dimashq) and Dar’a Governorate, cases of arbitrary detention and enforced disappearance were perpetrated with impunity. After years of living under siege, many civilians in areas recaptured by pro-government forces also faced numerous administrative and legal obstacles to access key services.
The foregoing violations and general absence of the rule of law paint a stark reality for civilians countrywide, including for 6.2 million internally displaced persons and 5.6 million refugees seeking to return. For these reasons, any plans for the return of those displaced both within and outside of the Syrian Arab Republic must incorporate a rights- based approach. In order to address effectively the complex issue of returns, the Commission makes a series of pragmatic recommendations for the sustainable return of all displaced Syrian women, men and children.
A report from Elizabeth Tsurkov in Ha’aretz confirms many of these findings. Describing Assad’s Syria as a police state with rampant poverty’ and a ‘playground for superpowers’, she writes:
Eight years into the crisis, Syria’s economy is in tatters, half of its population displaced, hundreds of thousands of Syrians are dead, many of Syria’s cities and towns lie in ruins. Yet on top of this pile of ashes Assad sits comfortably, quite secure in his grip on power.
In areas reconquered by the regime — or as the regime euphemistically describes it, areas that “reconciled” and whose residents “returned to the bosom of the nation” — the Syrian police state is back, more aggressive than ever…
In 2011, Syrians took pride in “breaking the barrier of fear.” But fear now prevails, as the various branches of the regime’s secret police launch raids and arrest suspected disloyal elements. Many of those arrested are former activists, rebels, health and rescue workers, and civil society leaders. Syrians who wish to prove their loyalty to the regime, obtain power through it or simply settle personal scores inform on others to the regime. Suhail al-Ghazi, a Syrian analyst based in Istanbul, told Haaretz that Syrians are informing on each other “because they have been doing it for years or because they need money or favors from the regime.” In areas recently recaptured by the regime, “some locals were always pro-regime and stayed there to work as informants or just could not leave. Now they have the chance to take revenge on the majority of civilians who apparently held a more favorable view of the opposition,” Ghazi explained.
Most of Syria’s population now lives below the poverty line. Across all parts of Syria unemployment rates are high, as the normal economy has been disrupted by years of war and the mass flight of businesspeople and capital out of the country. Syria’s middle class has largely disappeared — many of them fled to neighboring countries or Europe, while others are now living in abject poverty, along with most Syrians.
A small group of war profiteers linked to the various armed groups have been able to enrich themselves by trading in oil, weapons, antiquities, stealing aid, and smuggling people and goods in and out of the country and into besieged areas, while most Syrians struggle to survive. Nearly two-thirds of Syrians are dependent on aid for their subsistence. Basic services like electricity, cooking gas, clean water and health services are lacking in many parts of the country.
Speaking on the condition of anonymity, a resident of Latakia — an area where many of the regime’s leadership and their relatives reside — told Haaretz: “You have corruption everywhere. Bribing was common before the war, but now it is endemic.”
He described the ostentatious displays of ill-gotten wealth: “High-ranking officials, they and their families, have more rights. They roam the city in fancy cars and do whatever they want. Half of the country is dying from hunger, while the sons of officials are arrogantly showing off their wealth. With money you can do everything. This is not new, but it has become more obvious because of the lawlessness prevailing in Syria.”
At the sub-regional scale Enab Baladifiled a revealing report last month on conditions in the Ghouta (which it describes as ‘military-ruled ruins’):
Today, Ghouta is living in a state of siege similar to that it witnessed between 2013 and 2018 at the service, relief and security levels, but the difference is that food is available.
With dozens of announcements about the restoration of electricity to areas east of the capital, as well as the restoration of water and communication services, the needs of civilians are still not covered by those services repeatedly announced by the regime.
Enab Baladi spoke to five people from the eastern Ghouta who returned to it, all of whom refused to be identified for fear of the regime prosecution. They described the service situation as “miserable”, especially with regard to the water and electricity services.
According to the five sources, the electricity is continuously cut for five hours, operates for only one hour, and then it is cut again, while water reaches homes one hour a day, and people rely on submersibles and artesian wells which they dug during siege in the previous years to get water.
Some areas of Ghouta also lacked many of the services that were the top priorities of organizations before the regime forces controlled the region, while food today enters without manipulated prices, unlike in the past….
The report describes Eastern Ghouta as riven by checkpoints; an emphasis on demolition rather than reconstruction; and continuing arrests and detentions.
In early August [2018], al-Assad forces launched a campaign of arrests, which has been considered as one of the largest security operations since the regime took over Ghouta, for it has targeted the regime dissidents and activists in the Syrian revolution. The campaign was carried out in the cities and towns of Saqba, Hamuriyah, Duma, Mesraba, and Ein Tarma.
The regime also subjected local activists, civil society workers, and former media professionals, as well as members of local councils and relief agencies, to investigations into the aids they received when the area was held by the opposition.
Security branches launched arrest campaigns targeting members of the former “local council” and other members of Rif-Dimashq Provincial Council in the city of Kafr Batna in central Ghouta, according to Enab Baladi referring to local sources.
Sources affiliated to the council told Enab Baladi that Syrian security forces raided the houses and workplaces of the detainees before taking them to an unknown destination. Other local council members, who preferred to stay in Ghouta rather than go to northern Syria, are detained for the same reasons.
In the face of all that, it’s not easy to find grounds for optimism, but there is a glimmer of hope in a report from Maryam Saleh at The Intercept:
Syrian activists and lawyers are testing the bounds of international law, making two new attempts to bring the government of Bashar al-Assad before the International Criminal Court.
Syrian refugees in Jordan, through London-based lawyers, sent communications to the office of the ICC prosecutor, asking her to exercise jurisdiction over Syria based on a precedent set last year in a case involving Myanmar’s persecution of Rohingya Muslims. The communications are the latest push by Syrian civilians to hold accountable the government whose brutality upended their lives. In recent years, Syrian lawyers and human rights activists have experimented with rarely utilized aspects of international law, succeeding in getting European and American courts to weigh in on atrocities committed in Syria.
“Because of how politicized the war in Syria became, lawyers and those fighting for accountability really had to be creative,” said Mai El-Sadany, the legal and judicial director at the Washington-based Tahrir Institute for Middle East Policy. “The most recent ICC Article 15 submissions” — a reference to communications with the ICC on information about alleged international crimes — “are evidence of this, that there is space for creativity in the accountability space.”
She continues:
Even when the evidence of potential crimes exists, investigations into crimes committed in states that have not ratified the Rome Statute are near impossible because of jurisdictional issues, and U.N. Security Council members are quick to use their veto power to block investigations into crimes potentially committed by their allies.
That’s what makes the various avenues Syrians are pursuing so significant. As of last March, more than two dozen cases had been filed in European courts regarding atrocities committed by the Syrian regime, rebel fighters, and the Islamic State and other fundamentalist militant groups. The family of Marie Colvin, an American journalist killed in 2012 while reporting from the city of Homs, sued the Syrian government in a U.S. district court; in January, the court found Syria responsible for killing Colvin.
Many of the cases in Europe were brought under a legal doctrine known as universal jurisdiction; application of the doctrine varies from country to country, but it essentially allows for courts to prosecute cases regardless of where the crime was committed or whether the accused party has any links to the prosecuting state.
The biggest success so far has been in Germany, where authorities last month arrested a former high-ranking Syrian intelligence officer and two others who are accused of crimes against humanity for torturing detainees in Syrian prisons. Other cases remain pending in France, Sweden, and Spain….
These attempts are possible in part due to an unprecedented level of documentation of crimes in Syria. The victims in some of the cases were identified from a trove of 28,000 photos of people killed in Syrian detention centers, smuggled out of the country by a military defector codenamed Caesar. The U.N. General Assembly, in December 2016, took the step of creating the International, Impartial, and Independent Mechanism to investigate crimes in Syria since 2011. The IIIM, as the body is known, does not have independent prosecutorial authority, but it exists to collect information that could later be provided to courts or tribunals with jurisdiction over the crimes. Last year, 28 Syrian nongovernmental organizations committed to collaborating with the IIIM on its work.
This is heartening in its way, but whenever I’ve been asked about attempts to enforce accountability in relation to the systematic attacks on hospitals, I’ve had to say that the hideous intimacy between torturer and tortured allows for an identification and assignment of culpability that is much more difficult in the case of the extended ‘kill-chain’ involved in bombing.
But that doesn’t mean it’s impossible: we know, from the courageous work of activists cited in Maryam’s report, that Assad’s security apparatus fetishized record-keeping, and that many of those records have been smuggled out of Syria so that they can now serve as testimony and evidence (For other testimonies, see the work of Forensic Architecture on Saydnaya Prison that I described here: scroll down). To sharpen the point, hare some of the slides from a presentation I once gave around precisely these questions:
If my work on bombing in other theatres of war is anything to go by, there will also be extensive trails (paper or digital) that animated the air strikes: though how they can ever be exposed is another question.
I’m still converting my ‘Trauma Geographies‘ lecture into an essay – which has involved writing a prequel of sorts, ‘Woundscapes of the Western Front‘ – so, with my head buzzing with first-person accounts of trauma surgery on the front-lines, I was thrilled to see that David Nott has just published an account of his marvellous work in Syria (and many other conflict zones), War Doctor: Surgery on the Front Line (Pan Macmillan):
For more than twenty-five years, David Nott has taken unpaid leave from his job as a general and vascular surgeon with the NHS to volunteer in some of the world’s most dangerous war zones. From Sarajevo under siege in 1993, to clandestine hospitals in rebel-held eastern Aleppo, he has carried out life-saving operations and field surgery in the most challenging conditions, and with none of the resources of a major London teaching hospital.
The conflicts he has worked in form a chronology of twenty-first-century combat: Afghanistan, Sierra Leone, Liberia, Darfur, Congo, Iraq, Yemen, Libya, Gaza and Syria. But he has also volunteered in areas blighted by natural disasters, such as the earthquakes in Haiti and Nepal.
Driven both by compassion and passion, the desire to help others and the thrill of extreme personal danger, he is now widely acknowledged to be the most experienced trauma surgeon in the world. But as time went on, David Nott began to realize that flying into a catastrophe – whether war or natural disaster – was not enough. Doctors on the ground needed to learn how to treat the appalling injuries that war inflicts upon its victims. Since 2015, the foundation he set up with his wife, Elly, has disseminated the knowledge he has gained, training other doctors in the art of saving lives threatened by bombs and bullets.
If you’re unfamiliar with David’s extraordinary efforts in Syria, I touch on them – all too briefly – in ‘Death of the Clinic’ here. And the David Nott Foundation Facebook page is here.