
There are all sorts of ways in which the war on Syria has been a throwback to the First World War – and all sorts of differences too – but today brought news of yet another (and, unusually, a welcome one). Peter Walker reports for the Guardian:
The UK government is taking part in a pioneering international aid project which could see consignments of maggots sent to crisis zones such as Syria as a simple and effective way to clean wounds, it has been announced.
So-called maggot therapy has been used since the first world war, when their efficacy in helping wounds heal was discovered by accident, and it is sometimes used in the NHS, for example to clean ulcers.
The initiative, co-sponsored by the Department for International Development (DfID), will develop techniques to help people in conflict zones or areas affected by humanitarian crises to use maggots where other medical facilities might not be available, such as Syria and South Sudan.
Over at the Telegraph Sarah Newey adds:
Modern larvae treatment was developed following WWI after an American scientist, William Baer, noticed the benefits of maggots on soldiers wounds. Today the therapy is used in hospitals in developed countries, including the NHS, but they are yet to be used in war zones.
While photos of the maggots at work are unsavory, the treatment is highly effective.
Flies are reared in a lab, where their eggs are sterilised. The hatched maggots are then grown for a day or two, before they are applied to skin and soft tissue wounds either directly or in a biobag, which is wrapped around the injury.
Not only do the maggots remove dead tissue and flesh, but they control infection as their spit and saliva act as a natural disinfectant and promote healing. The maggots can be used to treat anything from burns to bedsores to gunshot wounds, and are left on an injury for two to four days.
The martial history of maggots is an interesting one.
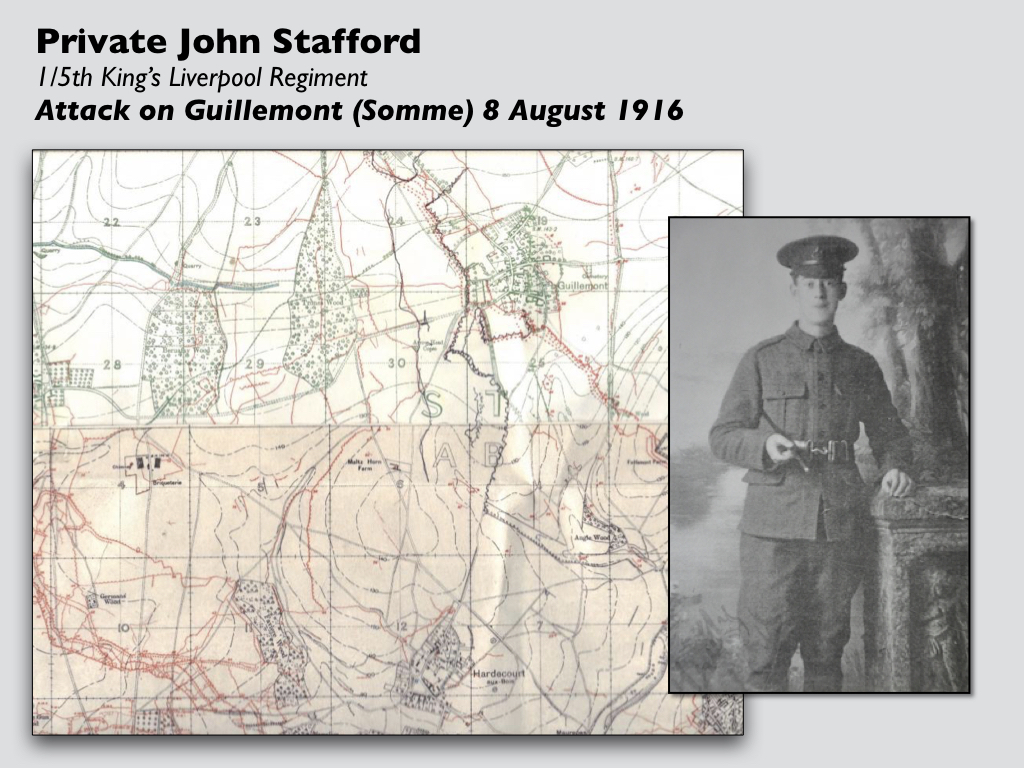
In ‘Trauma Geographies‘ I described the experience of one young soldier, John Stafford, who was wounded on the Somme in the early hours of 8 August 1916, and I’ll draw on that account here. He managed to crawl (and fall) into a shell-hole, where he examined his wound:
‘A bullet had passed through the flesh of the upper left thigh and entered the extreme inner high point of the right leg. The thigh bone was considerably shattered, the bullet having travelled downwards towards the knee. My field dressing was used and I lay flat again…’
There was no sign of rescue. His thirst increased as the sun climbed higher, but he knew nobody would venture out to rescue him until it was dark.
When night fell his hopes rose, though he was weak from loss of blood, but still nobody came. The next day the bleeding had stopped so Stafford removed the field dressing and to his horror ‘discovered that it was one mass of white grubs … I saw that my wounds were infested with maggots.’ Sickened, he hurled the heavy dressing away, but worse was to come:
‘Eventually the maggots spread over my leg from hip to knee and then settled on the other leg which was not so badly wounded. Occasionally I looked at their swelling rhythm, then finally turned away in disgust.’
He was eventually – and accidentally – rescued, but the maggots had probably already saved his life. In eating the damaged flesh they had performed a ‘natural’ debridement of the wound,

Stafford’s experience was by no means unique. It was not uncommon for wounded men to lie out in the open for days before they were recovered by stretcher-bearers, and often their wounds became infected – but the problem was bacterial infection not maggot infestation.

That same month (and in more or less the same place) Captain Lawrence Gameson was stationed with the RAMC’s 45th Field Ambulance in a shattered cellar at Contalmaison (above). It was a bruising experience;, and he said there ‘was hardly a part of the body I did not see cut or exposed’:
Maggot invasion was common. I can recall an unconscious man who arrived with part of a frontal lobe protruding through a hole in his skull. The protruding portion of brain was moving with maggots. When men had had to be left out wounded for some time, often their shoulders, buttocks or whole back were invaded by the creatures in the areas of skin compressed by the weight of their immobilised bodies. One man I saw had been lying out because both his legs were wounded. Prolonged pressure had caused necrosis of the skin over his buttocks and of the superficial portions of muscle beneath it. Maggots had invaded the deeper tissues. I had to pick them out with long forceps. The man was unaware of his condition. Maggot invasion was always accompanied by a foul smell, since it flourished only in tissues undergoing some degree of decomposition. As a rule, the victim did not notice the stink, or did not know that it came from his own body if sensitive enough to notice it.
The association of maggots with death, decay and decomposition was pervasive. Gameson described how he was called to extricate the body of a dead German soldier from a captured dugout:
He had fallen head foremost and was stuck there. On my preliminary examination in the dim light I could see only his field boots. I had come without my torch. Subsequently, on looking closer, I found that his flesh was moving with maggots. More precisely, I noticed that portions of his uniform were heaving up and down at points where they touched the seething mass below.
The smell was pretty awful. None of the men would touch him, although troops as a rule are not noticeably fastidious. The job was unanimously voted to me, because it’s supposed, quite wrongly, that doctors don’t mind. I went down the stairway with a length of telephone wire and lashed it round the poor chap’s feet. We hauled him up and dragged him away for some distance. The corpse left behind it a trail of wriggling, sightless maggots…
And yet, writing in the British Medical Journal on 3 March 1917 about the treatment of compound fractures, Captain Basil Hughes observed that ‘the presence of maggots in … wounds seems to exert an inhibitory action on the growth of the most virulent bacteria, and so acts beneficially. Maggots only thrive in dead tissue and seem to hasten its removal.’
This should have been – could have been – a crucial finding, for Hughes also emphasised that ‘all shell wounds are bound to become infected, whatever care be taken’, and listed ‘the bacteria most to be feared’. But it was those other associations – the smell of decay and the seething sight of the maggot-riddled bodies – that inhibited an appreciation of the therapeutic agency of maggots.
 As Sarah notes, William Baer (left) had made a similar observation while treating two soldiers also with compound fractures of the femur. These were among the most serious wounds of the war because the penetration of the skin by the bone made them peculiarly vulnerable to sepsis. In 1917, he wrote,
As Sarah notes, William Baer (left) had made a similar observation while treating two soldiers also with compound fractures of the femur. These were among the most serious wounds of the war because the penetration of the skin by the bone made them peculiarly vulnerable to sepsis. In 1917, he wrote,
‘two soldiers with compound fractures of the femur and large flesh wounds of the abdomen and scrotum [shades of Trey Parker] were brought into the hospital. These men had been wounded during an engagement and in such a part of the country, hidden by brush, that when the wounded of that battle were picked up they were overlooked. For seven days they lay on the battlefield without water, without food, and exposed to the weather and all the insects which were about that region. On their arrival at the hospital I found that they had no fever and that there was no evidence of septicaemia or blood poisoning. Indeed, their condition was remarkably good, and if it had not been for their starvation and thirst, we would have said they were in excellent condition. When I noticed the extent of the wounds, of the thigh particularly, I could not but marvel at the good constitutional condition of the patients. At that time the mortality of compound fractures of the femur was about seventy-five to eighty per cent…’
He continued:
‘I could not understand how a man who had lain on the ground for seven days with a compound fracture of the femur, without food and water, should be free of fever and of evidences of sepsis. On removing the clothing from the wounded part, much was my surprise to see the wound filled with thousands and thousands of maggots, apparently those of the blow fly. These maggots simply swarmed and filled the entire wounded area. The sight was very disgusting and measures were taken hurriedly to wash out these abominable looking creatures. Then the wounds were irrigated with normal salt Solution and the most remarkable picture was presented in the character of the wound which was exposed. Instead of having a wound filled with pus, as one would have expected, due to the degeneration of devitalized tissue and to the presence of the numerous types of bacteria, these wounds were filled with the most beautiful pink granulation tissue that one could imagine. There was practically no bare bone to be seen and the internal structure of the wounded bone, as well as the surrounding parts, was entirely covered with the pink, rosy granulation tissue which filled the wound. Bacterial cultures were made and, while one found a few Staphylococci and Streptococci still remaining, they were very few in number and not sufficient at that time to cause a pus formation. These patients went on to healing, notwithstanding the fact that we removed their friends which had been doing such noble work.’
Bauer drew on these findings to pioneer the use of ‘maggot therapy’ (myiasis) – but he did so at the Children’s Hospital in Baltimore ten years after the war ended. His first step was to grow maggots on raw meat ‘so he could observe their effect on destroying tissues,’ a colleague recalled, setting up the experiment in the hospital’s dining hall—’an unfortunate location for unwitting visitors’.

In fact, the use of maggot to treat wounds has an even longer history. They have been a common resource in many forms of indigenous medicine for thousands of years, and within a recognisably Western tradition Baron Dominique Larrey, Napoleon’s field surgeon (above), had observed their beneficial effects a hundred years before Bauer:
‘While the process of the suppuration of their wounds was going on, the wounded were much annoyed by the worms or larvae of the blue fly… These larvae are indeed greed only after putrefying substances, and never touch the parts which are endowed with life.’
Ironically, this was during the Syrian campaign (1798-1801).
