
This is the second in a new series of posts on military violence against hospitals and medical personnel in conflict zones. It examines the US attack on the Trauma Centre run by Médecins Sans Frontières (MSF) in Kunduz on 3 October 2015. I provided preliminary discussions here (on the conduct of US military investigations into civilian casualty incidents), here (on MSF’s own investigation into the attack), here (on the Executive Summary of the US military investigation), here (on two first-hand accounts from MSF personnel), here and here on the final report, and here (on the likelihood that the attack constituted a war crime). This post draws on those discussions but also on a close reading of the redacted report of the US military investigation [all page references refer to that report], on work by investigative journalists, and on ancillary materials and commentaries.
 One year ago today, in the early hours of the morning of 3 October 2015, a US AC-130U gunship (‘Spooky’) launched a concentrated attack on the Trauma Centre in Kunduz run by Médecins Sans Frontières. In an otherwise probing report on what happened, the Washington Post claimed that the gunship has sensors ‘that give it a “God’s eye” of the battlefield’. Here I explore some of the multiple ways in which such a view was – and remains – impossible. For militarized vision, like any other optical modality, is never a purely technical affair. A series of cascading technical errors bedevilled the US attempt to re-take Kunduz from the Taliban, who had swept into the city a few days earlier, but these were compounded by a series of profoundly human decisions and interactions and it was the intimate entanglement of the technical and the human that determined the hideous outcome.
One year ago today, in the early hours of the morning of 3 October 2015, a US AC-130U gunship (‘Spooky’) launched a concentrated attack on the Trauma Centre in Kunduz run by Médecins Sans Frontières. In an otherwise probing report on what happened, the Washington Post claimed that the gunship has sensors ‘that give it a “God’s eye” of the battlefield’. Here I explore some of the multiple ways in which such a view was – and remains – impossible. For militarized vision, like any other optical modality, is never a purely technical affair. A series of cascading technical errors bedevilled the US attempt to re-take Kunduz from the Taliban, who had swept into the city a few days earlier, but these were compounded by a series of profoundly human decisions and interactions and it was the intimate entanglement of the technical and the human that determined the hideous outcome.
At least 42 people were killed, including 24 patients, 14 medical staff and 4 caretakers. Many others were wounded and traumatized. Here is Dr Evangeline Cua, a Philippina surgeon who was on duty when the attack started:
We were like two headless chickens running in total darkness — me and the surgeon who assisted me in an operation. The nurses who were with us a moment ago had run outside the building, braving the volley of gunshots coming from above. I was coughing, half-choked by dust swirling around the area. Behind my surgical mask, my mouth was gritty, as if somebody forced me to eat sand. I could hear my breath rasping in and out. Layers of smoke coming from a nearby room made it hard to see where we were. Blinking around, I caught sight of a glow, from a man’s hand holding a phone. He seemed mortally wounded but was still trying to send a message…perhaps to a loved one?
I stood transfixed, not knowing where to turn or what to do. All around us, bombing continued in regular intervals, shaking the ground, sending debris sweeping and flying. One. Two. Three. I tried to count but there seems to be no abatement to the explosions. I stopped counting at eight and silently prayed that we could get out of there alive.
Fire licked at the roof at one end of the building, dancing and sparkling in the dark, reaching towards the branches of the trees nearby. The ICU was burning. Outside, only the constant humming from above pointed to the presence of something. An aircraft? Airstrike? Why the hospital? Why us? Then, without warning, another tremendous, ear splitting blast shook the building. The ceiling came crashing down on us and the last remaining lights were turned off, sending us to total darkness. I screamed in terror as wires pinned me to the ground. That was the last thing I could remember.

What follows is an attempt to answer those questions. It is fraught with uncertainty: the most detailed investigation to date has been carried out by the US military, but the redacted version of the final report that has been released to the public is (by the standards of other US military investigations) profoundly unsatisfactory – redacted with a brutishly heavy hand. Time and time again, ironically, references to the time of events have been removed; transcripts of radio communications and interviews by the investigating panel that have been released in other cases have been suppressed; and some redactions seem to have been made not for reasons of privacy or security but to avoid embarrassment (more here; you can download the report from US Central Command’s Freedom of Information Act (FOIA) library here).
All of this reinforces MSF’s original call for an independent investigation. I understand May Jeong‘s pessimism:
A former Afghan special forces commander who was at the command and control center in Kunduz during the fight assured me I would never get to the bottom of the attack. The reason why I couldn’t figure out exactly what had happened, he said, was the fog of war. “Ground truth is impossible to know. Even those who were there wouldn’t be able to tell you what they saw.”
But when the ‘fog of war’ – so often a convenient cover for all manner of horrors – is deliberately thickened – when visibility is ruthlessly reduced by redaction – then perfectly proper public interest is trumped by political and military expediency.
***
When the NATO-led combat mission to Afghanistan conducted by the International Security Assistance Force (ISAF) finished at the end of 2014 it was replaced by a much smaller advisory mission, Resolute Support, which was ‘to provide further training, advice and assistance for the Afghan security forces and institutions’. Resolute Support was authorized by a Status of Forces agreement between NATO and the Afghan government in Kabul. Its central hub was Kabul/Bagram, with four ‘spokes’ formed by four other ‘Train Assist Advise’ Commands to support four Afghan National Army Corps outside the capital (more here and here):
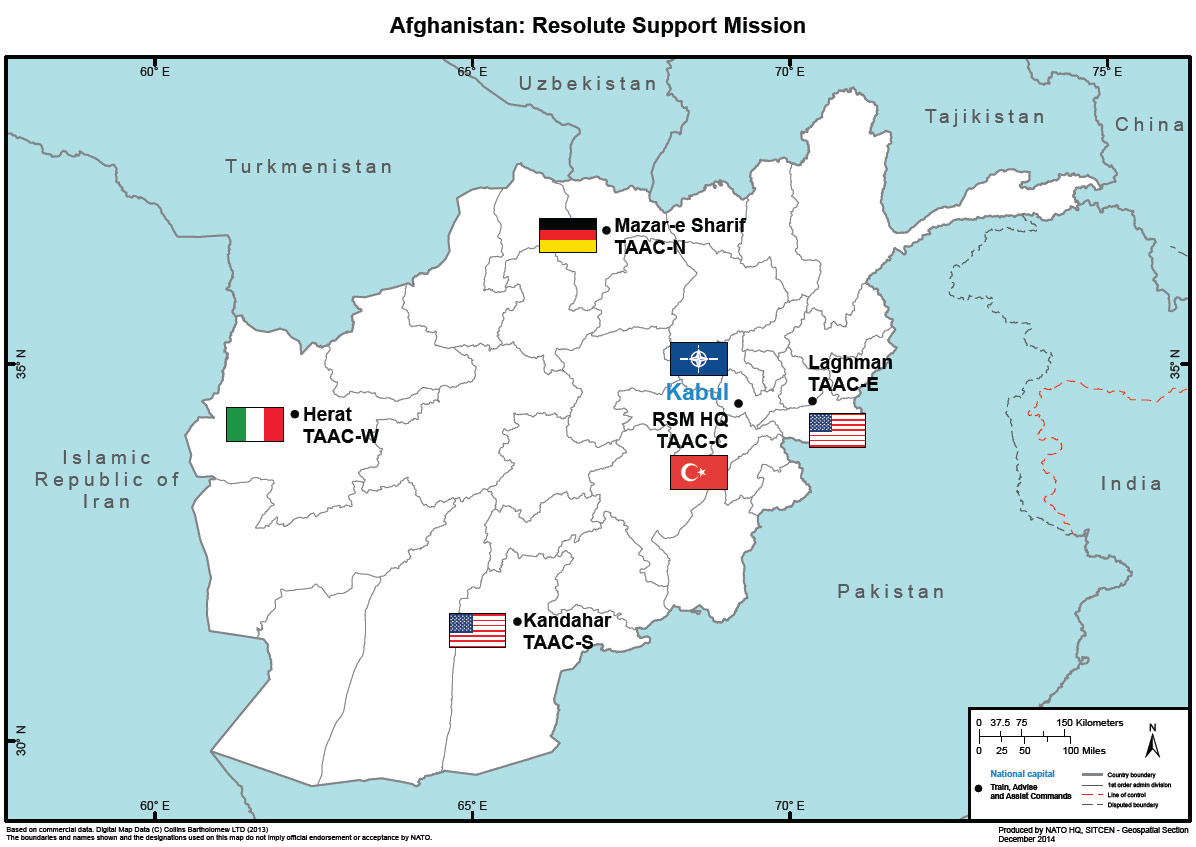
US troops were the major contributor to Resolute Support, but they were also assigned to the United States’s continuing (‘concurrent and complementary’) counter-terrorism mission now designated as ‘Operation Freedom’s Sentinel’. Until March 2016 both missions were under the overall command of General John Campbell.
By September 2015 the focus of US concern in Afghanistan was Helmand in the south – where the Taliban were on the ascendant, forcing Afghan government forces to retreat as they seized control of key districts and gained control of the Kajaki dam – and US Special Forces were rushed to Camp Bastion after the fall of Musa Qala gave the insurgents a strategic advantage.
By contrast, Kunduz in the north was regarded as ‘secure’ [135] after a series of combat operations at the start of the fighting season earlier in the year. As late as 13 August Brigadier-General Wilson Shoffner, Deputy Chief of Staff for Communications with Resolute Support, declared that although there had been ‘an attempt by the Taliban to try to stretch the Afghan security forces in the north’ the city of Kunduz ‘is not now and has not been in danger of being overrun by the Taliban’ (he also described the situation at Kajaki as merely a ‘local security challenge’). But those previous operations in Kunduz had targeted Taliban operations areas and did not extend to support zones outside the city.
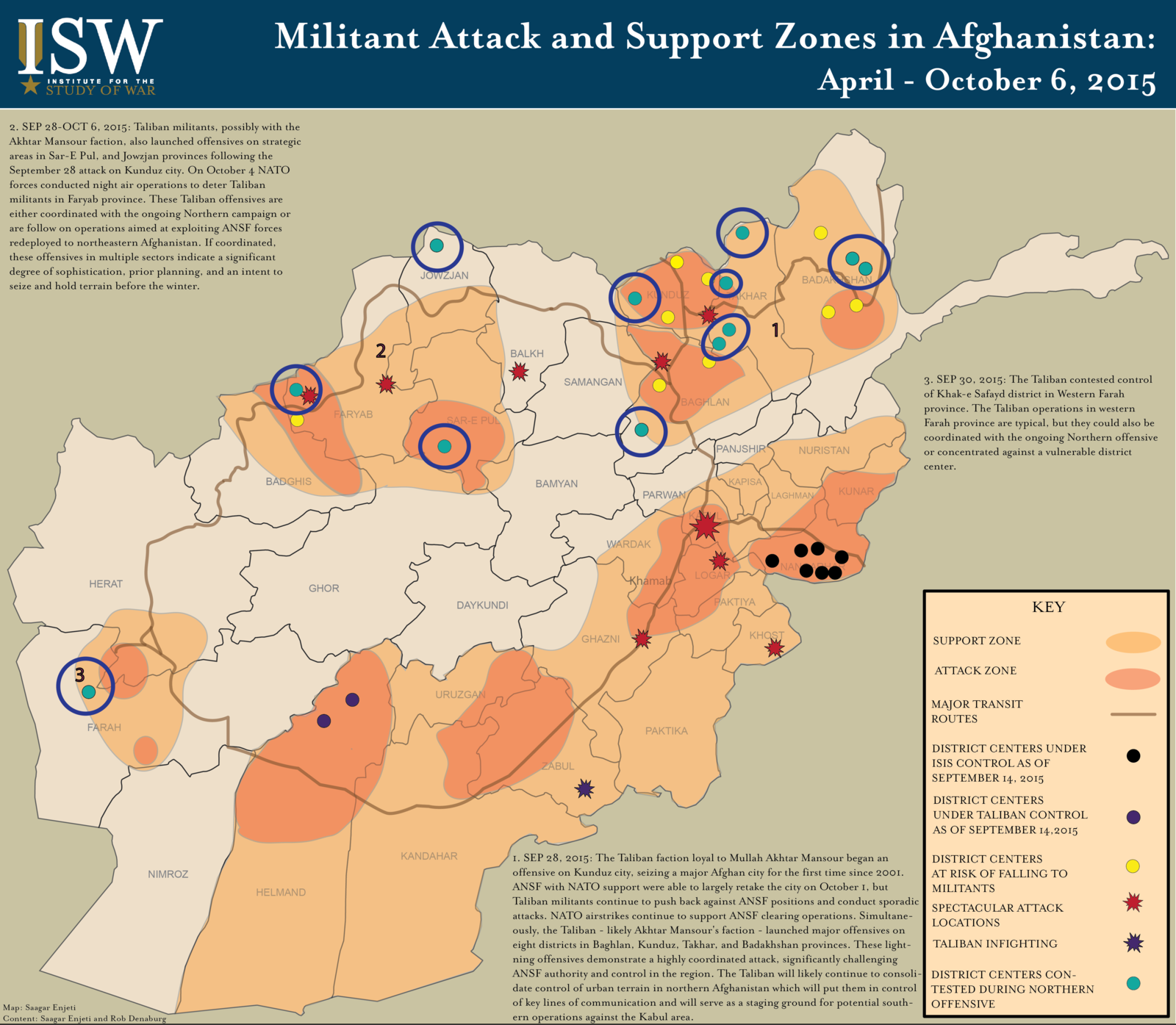
Obeid Ali reports that during the summer the Taliban continued to make inroads until they controlled areas to the south west, north west and south east of the city.
On 28 September 2015, the Taliban stormed various ANSF locations in Kunduz city from the three different directions they had spent so long preparing… The simultaneous attacks on the city and the collapse of check posts at the city ‘gateways’ destroyed the confidence of the ANSF inside the city in their ability to stand against this unexpected offensive. In the face of the well-organised and coordinated insurgent operation, most held out for only a few hours. A chaotic environment quickly spread and government officials, ALP [Afghan Local Police] commanders and some of the ANA [Afghan National Army] officers, fled to the military base at the airport [Camp Pamir], leaving Kunduz effectively leaderless.

Kunduz was a spectacular, strategic prize: the first city to fall to the mujaheddin in 1998 and the first time the Taliban had seized a major city since 2001, its capture signalled both a resilient Taliban and a faltering government footprint in the region.
•••
On 28 September there was a detachment of US Special Forces (‘Green Berets’) based at Kunduz airfield as part of the Train, Assist, Advise mission. Like every Operational Detachment – Alpha (OD-A) it consisted of just 12 soldiers, all cross-trained and capable of operating for extended periods of time with little or no support. On 29 September their superior command – the US Special Operations Task Force in Afghanistan – ordered two other OD-As to Kunduz. While they were in the air the OD-A on the ground sketched out a contingency plan (‘Kunduz City Foothold Establishment’) to assist the Afghan forces to return to the city and secure the Kunduz City Hospital and the Prison. There were repeated US airstrikes against Taliban positions in and around the city throughout the day, but by the time the OD-A reinforcements, together with other Afghan troops including Afghan Special Security Forces (below), arrived in the evening it was clear that the original plan was unworkable and their immediate priority had to be the defence of the airfield [032, 382].

The US reinforcements included Major Michael Hutchinson, who assumed overall command of the combined OD-As (he was identified as the Ground Force Commander by the New York Times). He had misgivings about the mission but accepted that ‘we can’t lose the provincial capital’ [377]. The next day a revised plan (‘Kunduz Clearing Patrol’) was submitted to the Special Operations Task Force for approval, which was granted that night, and the OD-As requested that Afghan Special Security Forces be accorded ‘designated special status’ that would permit the Green Berets to extend their own envelope of self-defence and assume a direct combat role (including calling in air strikes) to defend their partner forces if they came under attack [046-7].
By this time Médecins Sans Frontières had been in contact with both US and Afghan forces to ensure that they were aware of the location and status of its Trauma Centre in Kunduz. It was in the eye of the storm. Dr Kathleen Thomas, an Australian doctor in charge of the Emergency Room and the Intensive Care Unit, explained:
We all knew that at times, our hospital was in the middle of the rapidly changing front line – we could feel it. When the fighting was close – the shooting and explosions vibrated the walls. I was scared – we were all scared. When a loud “BOOM” would sound a bit closer to the hospital, we would all drop to the floor away from the large windows that lined the ICU walls. We also tried to move the patients and large (flammable) oxygen bottles away all from the windows, but the layout of the ICU prohibited doing this effectively. I worried constantly about the exposure from those windows – yet never thought to worry about the exposure from the roof.

Most of the patients were civilians. Of the combatants, MSF reported that most of them were from the Afghan army and police, as had been the case since the Trauma Centre opened, but once the city fell on 28 September ‘this shifted to primarily wounded Taliban combatants.’ The Afghan government speedily arranged the transfer of all its patients (apart from the most severely wounded cases) to another hospital.
By that night the Taliban announced that it was in control of the district. Kathleen Thomas described the scene:
The first day was chaos – more than 130 patients poured through our doors in only a few hours. Despite the heroic efforts of all the staff, we were completely overwhelmed. Most patients were civilians, but some were wounded combatants from both sides of the conflict. When I reflect on that day now, what I remember is the smell of blood that permeated through the emergency room, the touch of desperate people pulling at my clothes to get my attention begging me to help their injured loved ones, the wailing, despair and anguish of parents of yet another child lethally injured by a stray bullet whom we could not save, my own sense of panic as another and another and another patient was carried in and laid on the floor of the already packed emergency department, and all the while in the background the tut-tut-tut-tut of machine guns and the occasional large boom from explosions that sounded way too close for comfort.
Although the Trauma Centre had been on US Central Command’s ‘No-Strike List’ since October 2014 MSF now re-supplied its GPS coordinates and reminded the Ministry of Defence in Kabul that ‘MSF and its personnel observes strict neutrality and impartiality in the name of universal medical ethics and rights of populations affected by conflicts to humanitarian assistance’ and claimed ‘full respect of these principles and rules in order to be able to continue responding to the humanitarian and medical needs of all Afghans’ [144]. On 29 September MSF issued what would prove to be a remarkably optimistic statement:
We are in contact with all parties to the conflict and have received assurances that our medical personnel, patients, hospital and ambulances will be respected. With the government provincial hospital not currently functioning, MSF’s hospital is now the only place in Kunduz where people in need of urgent trauma care can receive it.
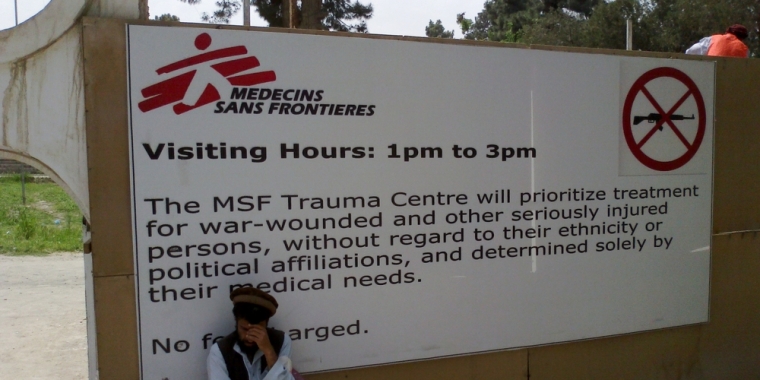
MSF had withdrawn from Afghanistan in August 2004 – after the targeted killing of five of its aid workers in June, the government’s failure to arrest those responsible, and Taliban threats to target organizations like MSF that they falsely claimed ‘work for US interests’ – and returned five years later with agreements from the US-led coalition, the Afghan government and the Taliban to respect the de-militarization of its hospitals (including a strict ‘no-weapons’ policy inside them). Initially MSF assumed responsibility for two public hospitals in Kabul and Helmand; two years later it opened its Trauma Centre in Kunduz inside the old Spinzer cotton factory. It soon became immensely important:
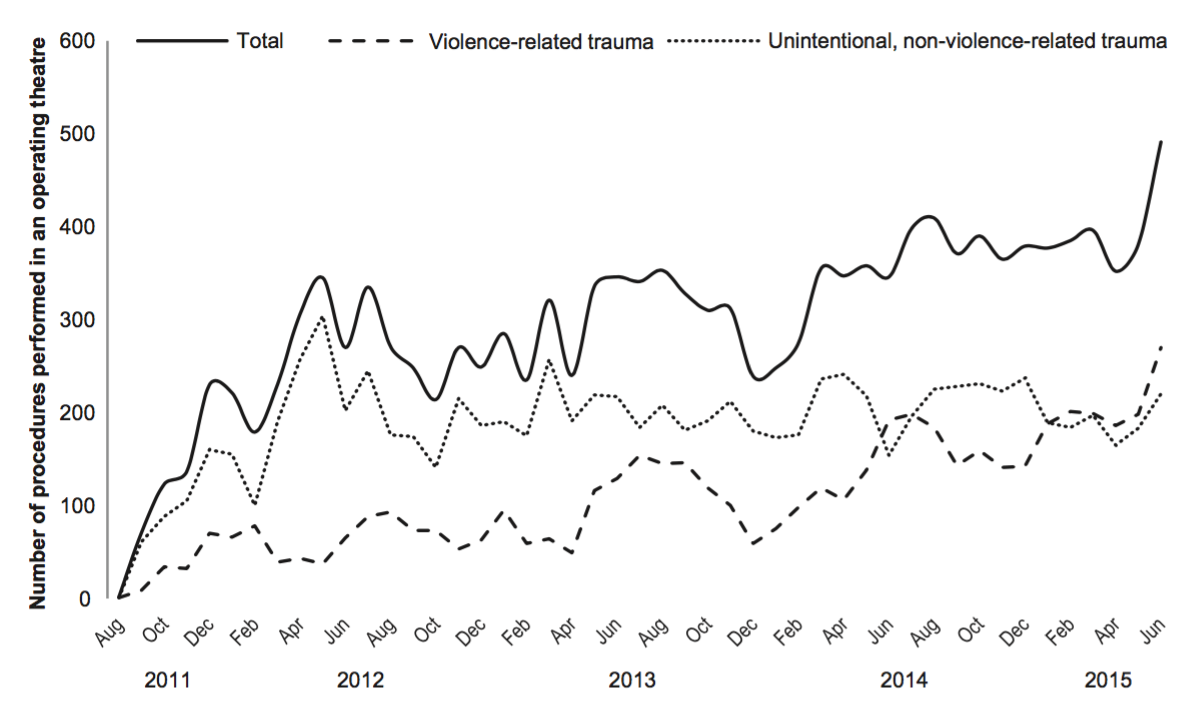
[Source: Miguel Trelles, Barclay T Stewart and others, ‘Averted health burden over 4 years at Médecins Sans Frontières (MSF) Trauma Centre in Kunduz, Afghanistan, prior to its closure in 2015’, Surgery (2016) in press]
Between August 2011 and August 2015 the Trauma Centre cared for 6,685 patients; roughly one-third were suffering from ‘violence-related trauma’, which included land mines and bomb blasts, gunshots, stabbings, assaults, rape and torture; one quarter of those were children. Procedures for complex wounds were the most common – debridement (excision), removed of shrapnel, care of burns – followed by orthopaedic procedures (including amputation). Those injuries increased dramatically in the months before the city fell to the Taliban. Miguel Trelles and his collaborators estimate that during this period the Trauma Centre averted 154, 254 ‘Disability Adjusted Life Years’; more prosaically:
The MSF Kunduz Trauma Centre provided surgical care for a large number of wounded and injured patients in the region. The surgical epidemiology is consistent with reports from other areas of prolonged insecurity in that unintentional, traumatic, non–war-related injuries generally outnumber those from violence. Nevertheless … the Trauma Centre provided surgical care for many adults and children injured directly by conflict (eg, injuries due to gunshots, land mines, bomb blasts). The health burden averted by surgical care at the Trauma Centre was large…
And yet, despite the importance of the Trauma Centre and its inclusion on a centralized No-Strike List that database was not consulted during the operational vetting and legal approval of the two plans drawn up by the OD-As [032, 045] (which, to be fair, had never been in the city and had no direct knowledge of the terrain; their Joint Terminal Attack Controllers had tried to print hard copy of ISR imagery before they set out from Camp Pamir but the base’s only printer was so old all it could produce were ‘giant magenta blobs’ that were completely useless [383] – so initially they relied on a single 1:50,00 map to plan and execute their operations [048]).
In fact – the irony is extraordinary – one member of the Special Operations Task Force testified that even they had no access to the No-Strike List and only discovered the existence of the Trauma Centre by accident, when ‘somebody was looking for additional medical facilities for use as emergency means to treat our own casualties’ if they could not make it back to Camp Pamir and the Forward Surgical Team based there [217, 219]. It was only then, late in the night of 29 September, that the Trauma Centre was added to the database maintained by the ISR [Intelligence, Surveillance and Reconnaissance] Tactical Controllers at the Special Operations Task Force at Bagram; early the next morning e-mails with this information were sent to ‘all ISR assets supporting operations in Kunduz’ [213].
***

On 30 September there was a secure videoconference between General Campbell, his Afghan counterpart and Major Hutchinson. It was clear that Campbell was exasperated at the conduct of the Afghan forces and attached great importance to re-taking the city. Fired up, Hutchinson briefed his men on the planned Kunduz Clearing Patrol, relaying the spirit of Campbell’s comments and telling them this was ‘a no fail mission’, that ‘all of the civilians have fled and only the Taliban are in the city’, and that ‘everything is a threat’ [256]. That night, once the mission had been approved, the Green Berets fought their way into the city alongside the Afghan Special Security Forces, with Close Air Support from US aircraft including an AC-130 gunship that ‘continuously called out and engaged [Taliban] ambush sites’ [325]. This seems to have been the same aircraft and crew that returned on 2/3 October; the sensor operator described that fateful mission as their third flight over Kunduz, following two others on 2 September and 30 September, the last when they provided armed overwatch for a US convoy into the city centre and engaged the Taliban at multiple locations. Indeed, he claimed that those previous missions had provided them with ‘good situational awareness’ of Kunduz and the ‘patterns of life’ of both civilians and insurgents [362].
Before dawn on 1 October the US and Afghan troops had cleared several key buildings and established a defensive strongpoint in the Provincial Chief of Police Compound [PCOP]. They hunkered down and came under repeated mortar, rocket-propelled grenade and automatic weapons fire, and throughout that day and the next their Joint Terminal Attack Controller called in multiple strikes from F-16 aircraft, many of them ‘danger close’, in immediate proximity to the PCOP [332].

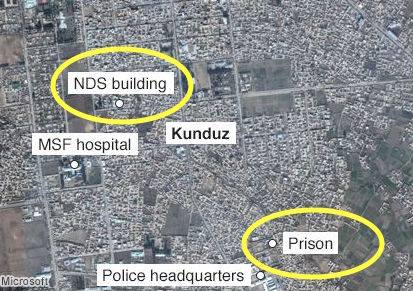
By the end of the afternoon on 2 October several Afghan troops had been wounded. Their commander was all for taking the casualties back to Camp Pamir immediately, but Hutchinson persuaded them that this was madness: they were stable so the medical evacuation should wait for the cover of darkness. The Afghan Special Security Forces agreed; while they were at Pamir they would re-supply and then return to attack a command and control centre they said had been established by the Taliban in the National Directorate of Security compound (NDS) to the south west of the PCOP which the Afghan SSF also referred to as ‘the NDS prison’ [386-8]. The investigation report includes this map showing the relationship of the PCOP to the NDS Compound and the MSF Trauma Centre:
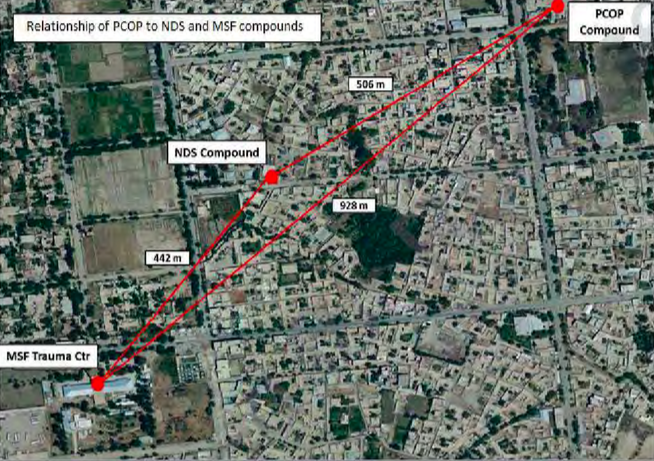
[A similar map included in a detailed analysis by The Intercept mis-locates the PCOP – almost certainly confusing it with the NDS Prison that the Operations Center in Bagram wrongly assumed was the intended target of the air/ground operation: see below]
The Afghan Special Security Forces were assured that Close Air Support would be extended to the convoy once they had returned to the ‘self-defence perimeter’ beyond the PCOP – a ‘bubble’, Hutchinson called it, roughly defined by the range of the heavy machine guns and anti-aircraft guns used by the Taliban [387].
But by then the F-16s providing close air support were running low on munitions and in the early evening, with the situation in Kunduz remaining precarious, the Special Operations Task Force scrambled the AC-130 gunship from Bagram to take over.
***
The AC-130 (call-sign ‘Hammer’) was a mission in a hurry and the aircraft took off without a proper briefing or any geospatial intelligence products. All the aircrew had was the grid location of the PCOP and the call sign and contact frequency for the OD-As [052]. By then, superior commands had received the e-mail detailing the location of the Trauma Centre, and at 1847 the Fires Officer from Combined Joint Special Operations e-mailed a package of ‘mission products’ to the Electronic Warfare Officer onboard the AC-130 which included that information. But en route to Kunduz one of the aircraft’s communications systems failed and the message never arrived; when the aircrew did not acknowledge receipt, the Fires Officer at Bagram made no attempt to pass the information over the radio (which was working) [052].
At 0130 on 3 October the Afghan convoy left on its evacuation and re-supply mission, and Hutchinson contacted the AC-130 through his Joint Terminal Attack Controller (JTAC) to ask them to carry out a ‘defensive [infrared] scan’ of the area of operations. Specifically, he wanted to prepare the ground ahead of the convoy’s return: if they were ambushed and ‘got fixed in place what I wanted to do was to reduce heavy weapons and strongpoints so that they would be able to effectively maneuver on to the objective’ [390]. To that end he supplied the aircraft with a grid location for the NDS compound.
It is unclear – from the redacted report, at least – how the co-ordinates of the target were obtained. Hutchinson said that when the Afghan Special Security Forces showed him their plan for securing the NDS compound it included ‘a grid [which] said, I think, NDS prison’, but when he plotted the location he realised it was not the Prison to the south that was one of the objectives included in the original plan to establish a foothold in the city. Hutchinson riffed on the multiple NDS facilities throughout Kunduz, but this begs a crucial question: how did he plot the grid to confirm the location? He claimed to have been working from the 1:50,00 map spread out on the hood of his armoured vehicle, which could hardly have provided the co-ordinates required for a precision strike. The Joint Terminal Attack Controllers would have had access to digital imagery stored on their laptops, but by this stage they were running low on batteries and cannibalising the radios of other Green Berets to keep communications with the AC-130 open [334, 383]. ‘The worst part of it,’ Hutchinson said, was that the day after the strike they found a detailed 1:10,000 map produced by a Provincial Reconstruction Team in 2013 ‘with nice crisp imagery, and it had everything labelled with 10-digit grids’ [397]. The commanders of the other two OD-As remembered it differently, both testifying that the map was found in the provincial governor’s office on 1 October.

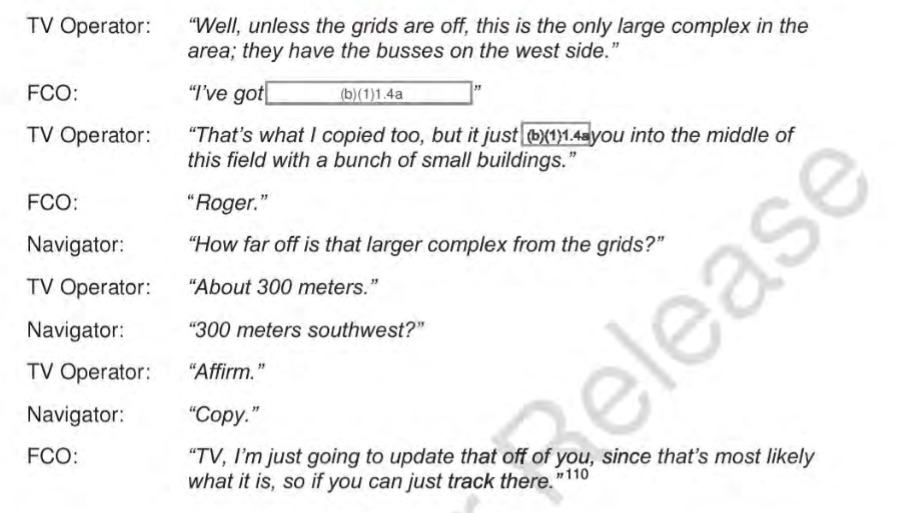
All this matters because when the TV sensor operator on the AC-130 (above) inputted the grids that were passed by Hutchinson via his JTAC he found ‘it put me in a field with residential buildings’. The AC-130 has a sophisticated sensor suite, including high resolution sensors (an All Light Level Television system, infrared detection set and strike radar to permit all weather/night target acquisition). But reading between the redactions in the investigation report there is some suggestion that there are also known technical issues with the system (perhaps distortion introduced by the aircraft’s height and/or orbit, because the AC-130 had been forced out of its overhead orbit at 2220 by taking evasive action against a surface-to-air threat): ‘Nothing in the immediate location matched the target but from training I was aware that at significant [redacted]…’ [363].
So the sensor operator widened the search and found a large compound 300 metres to the south that appeared to match the description of the target. It was not difficult to find: the Trauma Centre had its own generator and was the only building in the city that was still brightly illuminated. At first sight the sensor operator said ‘there was nothing else near the original location that could match the description of a prison.’

‘As we got closer,’ s/he continued,
I observed multiple [redacted: this is surely MAMs or ‘military-aged males’, a term the US military was supposed to have discontinued, which would explain the otherwise puzzling deletion] walking in between buildings [redacted] entrances with [redacted: guards?] posted. After passing back the information to the JTAC he said the compound was under enemy control and that those [redacted: MAMs?] were declared hostile [363].
The navigator had informed the JTAC that the grids had originally plotted to the middle of a field but they now had a large compound in their sights, a T-shaped structure with an arch gate and nine people ‘roaming outside’. The Green Berets conferred with the Afghan Special Security Forces in the PCOP who confirmed that this was the NDS compound, and the Fire Control Officer on the AC-130 adjusted the target location in the fire control system accordingly [054, 242].
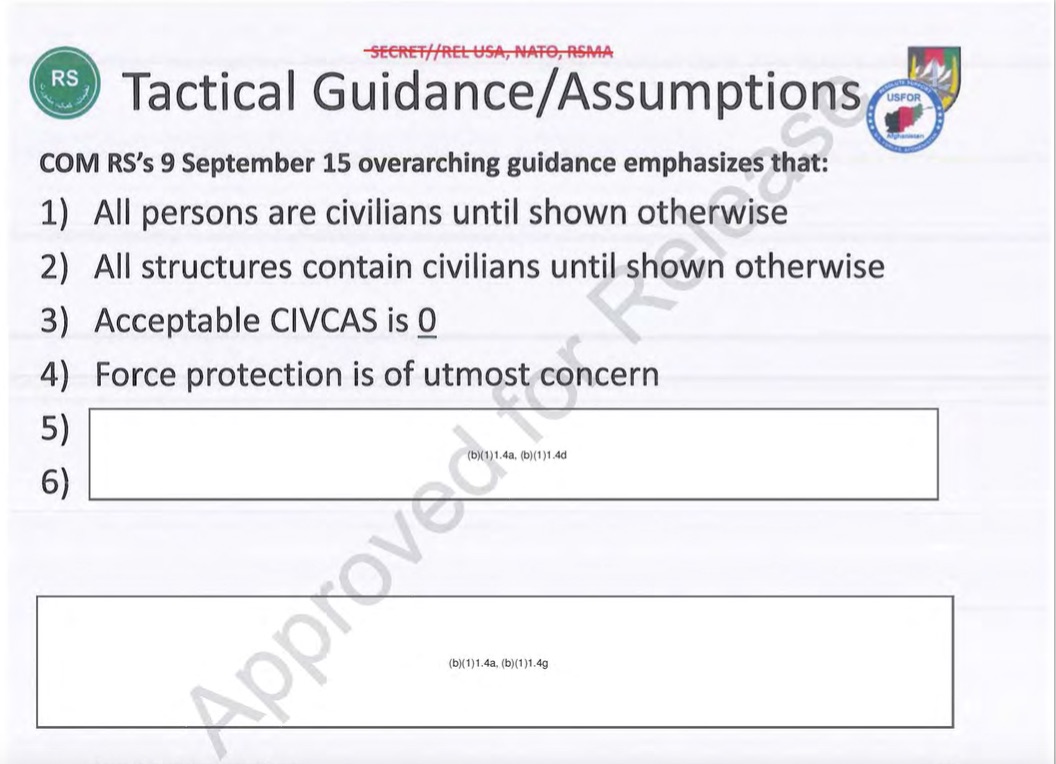
But the sensor operator, more mindful of the Tactical Guidance issued by General Campbell (below), testified that he wanted ‘to make sure we were not inadvertently declaring civilians hostile’.
So he re-entered the original co-ordinates (‘to determine any system [redacted: error?]’) – by then the AC-130 had moved to a more accurate, overhead orbit [057] – and this time the sensor homed in on a second compound:
a much smaller compound with two large buildings, what appeared to be a third smaller shack, two overhangs, a wall surrounding, what appeared to be guard towers at the four corners with a single entrance on the south side of the compound and was unable to observe any movement in that compound [363].
This underscored his concerns. ‘Now that we are closer,’ he told the rest of the crew,
even though that compound [is] the only one that’s limited and has activity, if you look in the TV’s screen you can see this hardened structure [the second compound] that looks very large and could also be more like a prison with cells. So I just want to verify that before we start declaring people hostile, that we are 100 per cent sure that this is the correct compound [057].
He asked the navigator to request a more detailed target description from the Joint Terminal Attack Controller (though the JTAC was not told that the aircraft’s sensors had now identified two different compounds from the same grids).
The JTAC came back with a target description of multiple buildings with a wall surrounding, and a main gate with an arch shape. I asked for further clarification on which side of the compound that gate was on, to which he replied the North side of the compound. The gate I was able to make out at the first compound was on the north side and matched the target description [363].
The first compound was the MSF Trauma Centre; the second was the NDS compound.
***
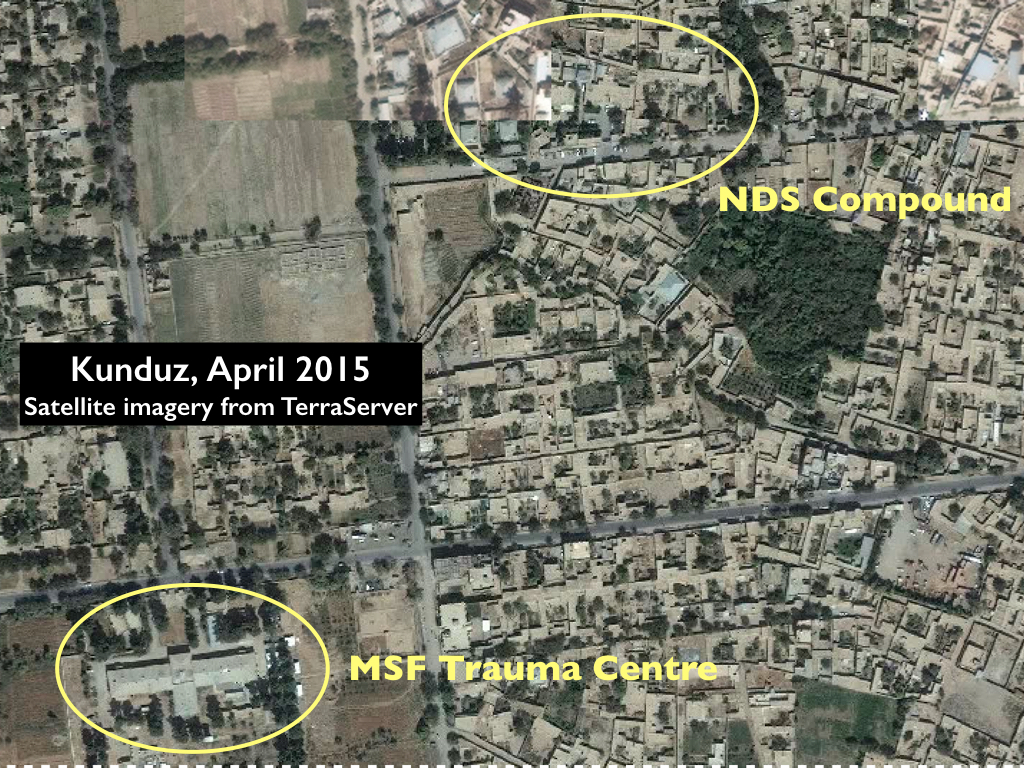
The redacted version of the investigation report includes a satellite image of the MSF Trauma Centre but conspicuously failed to include a corresponding image of the NDS compound. Yet from TerraServer’s satellite imagery (below) it is clear that the two are radically different, and in fact the gate on the NDS compound faced south not north.


Neither Hutchinson nor his JTAC had access to real-time imagery from the AC-130 because the same antenna that prevented the aircraft receiving the e-mail with the No-Strike List also prevented it from transmitting a video feed to the JTAC’s laptop, and so both the aircrew and the US forces on the ground had to rely on verbal descriptions. The investigation report calls the characterisation of the target building ‘a vague description’ [034] but, as Mathieu Aikins pointed out in a superb analysis of the strike, ‘it’s actually a rather specific description that corresponds to MSF’s distinctive layout.’ Indeed, when the aircrew compared the two compounds they were persuaded by the description of a ‘T-shaped structure’ that they had identified the correct target.
Once the AC-130 aircrew’s description of the Trauma Centre had been confirmed by the Afghan Special Security Forces as the NDS compound, the circle was closed. As Hutchinson testified, he had a report from the AC-130 ‘that describes a target, the disposition of the target and the pattern of life on it that’s completely consistent with what I’ve heard from the Afghans…’ Whether the Afghans deliberately substituted a description of the Trauma Centre for the NDS compound remains an open question. From their own (separate) interviews in Kunduz, both May Jeong and Mathieu Aikins repeatedly raise this as a distinct possibility. Some informants insisted that the Trauma Centre had been overrun by the Taliban, confirmed (so they said) by raw intelligence and communications intercepts, even that it was being used as a firing position – a claim that was repeated by the government in Kabul in the immediate aftermath of the strike – while others complained that MSF treated Taliban casualties who then returned to the fray: ‘patching up fighters and sending them back out.’ Much of this is ex post facto rationalisation; clearly many Afghans regarded the attack on the Trauma Centre as perfectly justified. But Aikins asks a more pointed question: Did Afghan forces, out of longstanding mistrust of MSF, draw the United States into a terrible tragedy?’
If they did, then it had to have been a spur-of-the-moment decision to take advantage of a developing situation, since the Afghan Special Security Forces had originally provided the correct grids for the NDS compound.
More telling, I suspect, is that from 0100 until well into the attack on the Trauma Centre the only people who had the co-ordinates for the target now in the sights of the AC-130 were the aircrew, who did not pass the grid location for what they had incorrectly identified as the target back to Hutchinson. And yet the ground force commander had already told the navigator he had ‘great confidence in the grids passed [057]’, and it is astonishing that this did not prompt a more extensive discussion among the aircrew since the original grids had plotted first to an open field and second to the NDS compound but never to the Trauma Centre that had now been designated as the target.
Neither did the aircrew pass the revised grids back to the Special Operations Task Force who were monitoring events from Bagram. Repeating Hutchinson’s earlier mistaken assumption, the staff in the Operations Center at Bagram believed the target (‘the NDS prison’) was the Prison in the south of the city which had been included in the original Kunduz City Foothold Establishment plan, and they tasked an MQ-1 Predator to provide surveillance over that location [059].
Hutchinson could not view the video feed from the Predator, since the laptops in the PCOP were desperately short of batteries, but the Special Operations Task Force did have access to the drone’s real-time imagery. Nothing was happening around the Prison, and confident that this was the strike location nobody at Bagram attempted to confirm the coordinates until the attack on the Trauma Center was well under way. At 0207 they heard a sudden, direct transmission from the AC-130 – ‘unreadable numbers followed by going hot/rounds away’ – and ‘the quickness of the going hot call’ suggested to one experienced JTAC at Bagram that ‘there was possibly a dire situation on the ground.’ But ‘the passing of engagement grids was broken, unreadable’, and s/he immediately ‘made multiple attempts to get a resend of [the] grid of engagement’. Those requests ‘were either not acknowledged or met with “still engaging/hot”‘, but this was ‘not uncommon due to the task saturation during coordination and employment by ground JTACs and aircraft’. Meanwhile another JTAC in the Operations Centre, realising that ‘no activity was noted at the facility’ – presumably by the Predator on station over the Prison; the Taliban had reportedly freed all the prisoners when they took the city – tasked the Predator crew to ‘find the engagement area’ [261-4]. At 0220 they were successful, and once the new grids had been checked the Operations Center realised that the AC-130 was attacking the Trauma Center.
***
Hutchinson provided two contradictory rationales for the attack. One was offensive: his JTAC relayed to the AC-130 that Hutchinson’s intent was to ‘soften the target’ (meaning the NDS compound) for the Afghan convoy returning from Camp Pamir. When the aircrew asked for clarification they were told they were to ‘destroy targets of opportunity that may impede partner forces’ success’ [059]. When he was questioned by the investigating officers, Hutchinson represented this as pre-emptive and precautionary: ‘If they were going to take contact I did not want to play twenty questions while they were taking fire’ [391]. The other was unambiguously defensive: the immediate trigger for Hutchinson to clear the AC-130 to open fire was the sound of automatic gunfire from the east-west road near the NDS compound.
What did it for me in the end was when I believed the [redacted] convoy to be at that parallel cross street … or the perpendicular cross street … to the facility, I heard sustained automatic weapons fire … and it was coming from that general direction. And so I asked the [redacted] are they in contact yet. He can’t get through [to] them at first, and so I think okay, so that’s a sign they’re probably in contact… Fire continues and I ask him again and he says strike now, assume they are decisively engaged’ [393-4].
It’s not clear from the redactions who Hutchinson was talking to, but it was almost certainly someone from the Afghan Special Security Forces in the PCOP. What is certain – and known to the aircrew on the AC-130, who were also tracking the convoy, but not to Hutchinson – was that the convoy was nowhere near the NDS compound or even the Trauma Centre at that time but 9 km away, still within the northern perimeter of the airfield.
Hutchinson’s attention was on the sound of gunfire. He explained that most of the fire directed against his forces in the PCOP compound had been from the west, and it was ‘unthinkable’ that ‘there would have been anything functional over there in terms of essential services’ [394] – like a hospital.
And so, at 0202 Hutchinson had his JTAC instruct the AC-130 to strike the ‘objective building first’ and then to provide ‘suppressing fire’ (which the JTAC later described as a ‘PAX cocktail’ and the aircrew translated as ‘MAMs’ [military-aged males]). Again the aircrew sought clarification; they wanted to be sure that their target was the ‘large T-shaped building in the centre of the compound’ and that ‘we are [also] cleared on people in this compound.’ It was and they were; at 0208 the first round was fired as the Electronic Warfare Officer announced the grids over the radio: the garbled transmission received at Bagram [064-6].
***

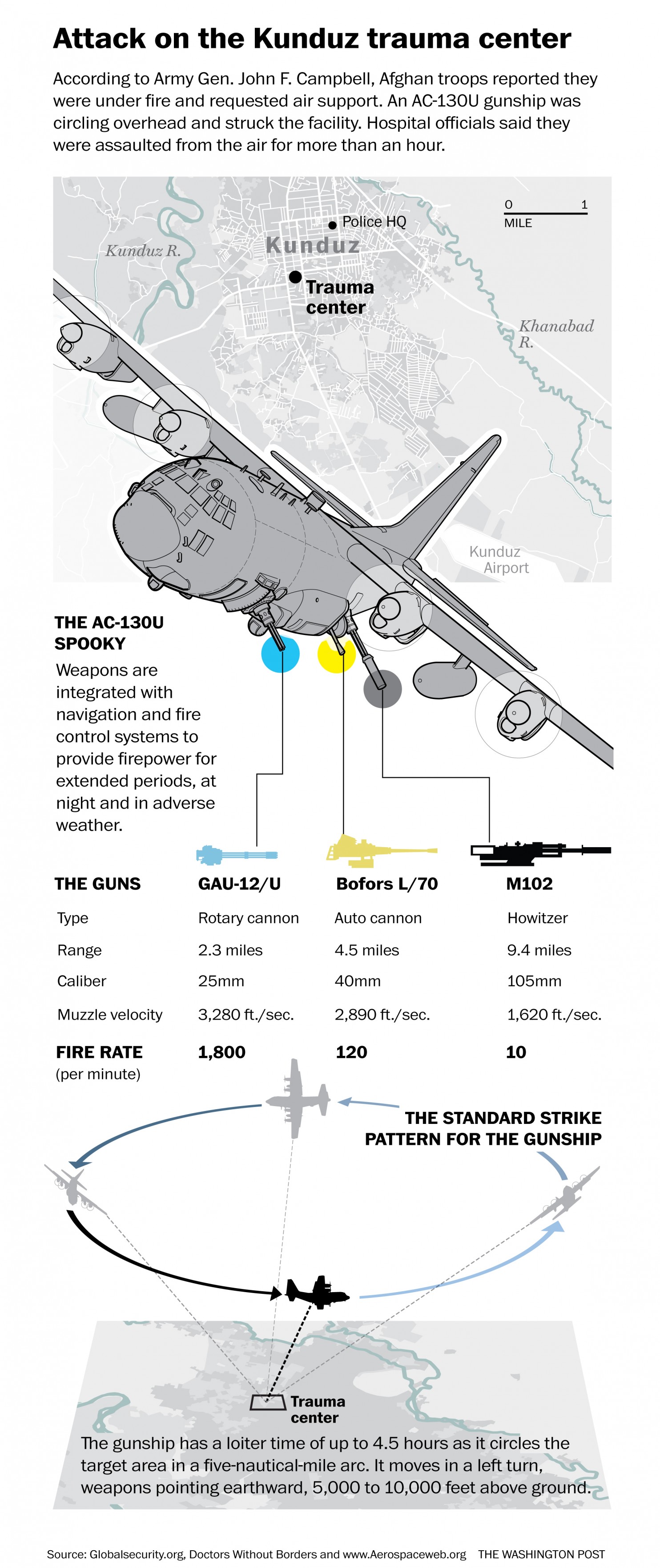
The AC-130 made five passes over the Trauma Centre at 15-minute intervals, firing a total of 211 rounds. But ’rounds’ fails to convey the scale of the ordnance involved. As May Jeong notes, the AC-130 is ‘built around a gun’; it is, after all, a gunship. It has a 105 mm M102 Howitzer that fires high explosive shells at 10 rounds a minute (reputedly the largest gun ever operated from a US aircraft); a 40 mm Bofors cannon that fires 120 rounds a minute; and a 25mm 5-barrelled Gatling cannon that fires incendiary rounds at 1,800 rounds a minute. YouTube has a video of a live-firing exercise carried out by the 4th Special Operations Squadron in 2016 that is truly chilling:
All these weapons are side-firing; the AC-130 performs a slow left-banking pylon turn in a five-mile orbit to keep its weapons on target for much longer than a conventional strike aircraft:
The results on the ground were catastrophic.


All the patients in the ICU died except one, alongside the caretakers who were with them; one doctor, three nurses and a cleaner who were in the ICU were also killed. Here is Kathleen Thomas again:
I hope with all my heart that the three sedated patients in ICU, including our ER nurse Lal Mohammad, were deep enough to be unaware of their deaths — but this is unlikely. They were trapped in their beds, engulfed in flames.
The same horror that rocked the ICU rocked the rest of the main building as the plane hit with alarming precision. Our ER nurse Mohibulla died. Our ER cleaner Najibulla died. Dr. Amin suffered major injuries but managed to escape the main building, only to then die an hour later in the arms of his colleagues as we desperately tried to save his life in the makeshift operating theater set up in the kitchen next to the morning meeting room. The OT nurse, Abdul Salam, died. The strikes continued further down the building, tearing through the outpatients department, which had become a temporary sleeping area for staff. Dr. Satar died. The medical records officer Abdul Maqsood died. Our pharmacist Tahseel was lethally injured. He also made it to safety in the morning meeting room, only to die soon after, having bled to death. Two of the hospital watchmen Zabib and Shafiq also died.
Our colleagues didn’t die peacefully like in the movies. They died painfully, slowly, some of them screaming out for help that never came, alone and terrified, knowing the extent of their own injuries and aware of their impending death. Countless other staff and patients were injured; limbs blown off, shrapnel rocketed through their bodies, burns, pressure wave injuries of the lungs, eyes, and ears. Many of these injures have left permanent disability. It was a scene of nightmarish horror that will be forever etched in my mind.

***
The loss of life and the destruction of the hospital was appalling. But the effects of the air strike have reverberated far beyond the Trauma Centre and the events of 3 October. In February this year Sophia Jones told the troubling story of a father of four who lost his right arm and the sight of one eye when he was caught in cross-fire between the Taliban and the Afghan army. With the destruction of the Trauma Centre in Kunduz there were no local hospitals capable of treating his life-threatening injuries, and it took him two agonising days to travel 200 miles to the Surgical Center for War Victims run by another NGO, Emergency, in Kabul – now ‘the only free, specialized trauma hospital of its kind treating war victims in Afghanistan.’ Like MSF, Emergency is absolutely clear that ‘we cannot be on one side of the war’: ‘a patient is a patient’. Like MSF, most of Emergency’s patients are civilians. But, as Luke Mogelson found in the spring of 2012,
At Emergency’s hospital in Kabul, it’s not unusual to find Afghan national security forces recovering in the same ward as Taliban insurgents, and after a while, the ideas that make enemies of the two men lose their relevance; the daily spectacle of their impact on human bodies invalidates them.
That was then. ‘After Kunduz’, Emergency’s program co-ordinator now concedes, ‘anything is possible.’ It would be truly, desperately awful if one of the casualties of the air strike on the Trauma Centre turned out to be the core principle of medical neutrality.
One year after Kunduz, Christopher Stokes, MSF’s General Director, warned that ‘A war without limits leads to a battlefield without doctors.’ MSF pledged not to allow that to happen. They must not stand alone.
To be continued

Pingback: The exception to the exception | geographical imaginations
Pingback: Underground medicine | geographical imaginations
Pingback: Striking Syria | geographical imaginations
Pingback: The Death of the Clinic | geographical imaginations
Pingback: ‘Your turn, doctor’ | geographical imaginations
Pingback: Fighting over Kunduz | geographical imaginations
Pingback: Spaces of exception and enemies | geographical imaginations