I’m continuing to work on attacks on hospitals and health care workers in conflict zones – see ‘The Death of the Clinic’ here for a general discussion – and I’ve just finished reading the preliminary report on the weaponisation of health care from The Lancet-American University of Beirut Commission on Syria. You can find out more on the Commission here and download the open access report here.
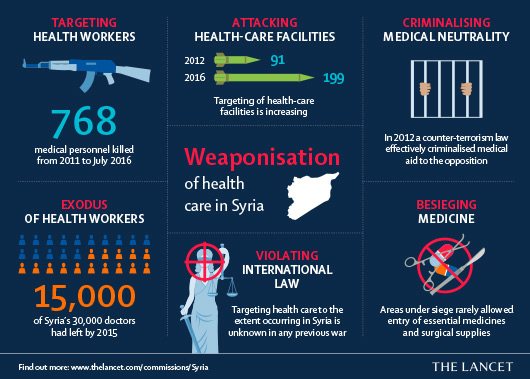
The authors propose the ‘weaponisation of health care’ to capture ‘the phenomenon of large-scale use of violence to restrict or deny access to care as a weapon of war’:
Weaponisation is multi-dimensional and includes practices such as attacking health-care facilities, targeting health workers, obliterating medical neutrality, and besieging medicine. Through large-scale violations of international humanitarian laws, weaponisation of health care amounts to what has been called a “war-crime strategy”. Weaponisation of health care in the Syria conflict is manifested most notably in the targeting of health workers and facilities.
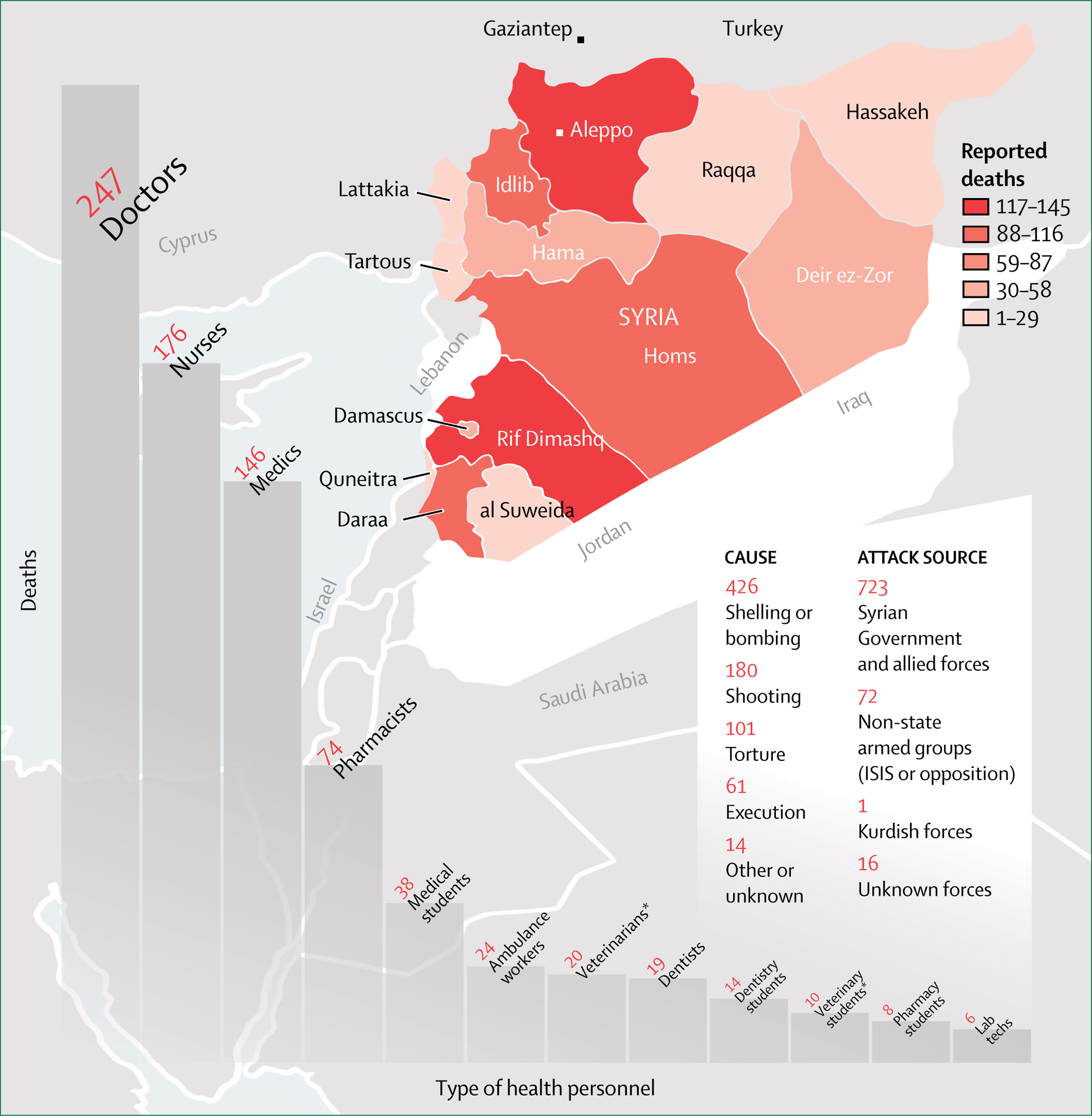
They trace the targeting of health-care workers by pro-government forces in Syria back to the earliest weeks of protest against the regime, but the ‘substantial militarisation’ that followed – especially after the ‘military surge’ that began in September 2015 when Russia joined the Syrian government forces – made those attacks ever more aggressive and ever more systematic. This map, based on the work of Physicians for Human Rights, provides a minimal accounting of attacks on doctors, nurses and other healthcare workers:
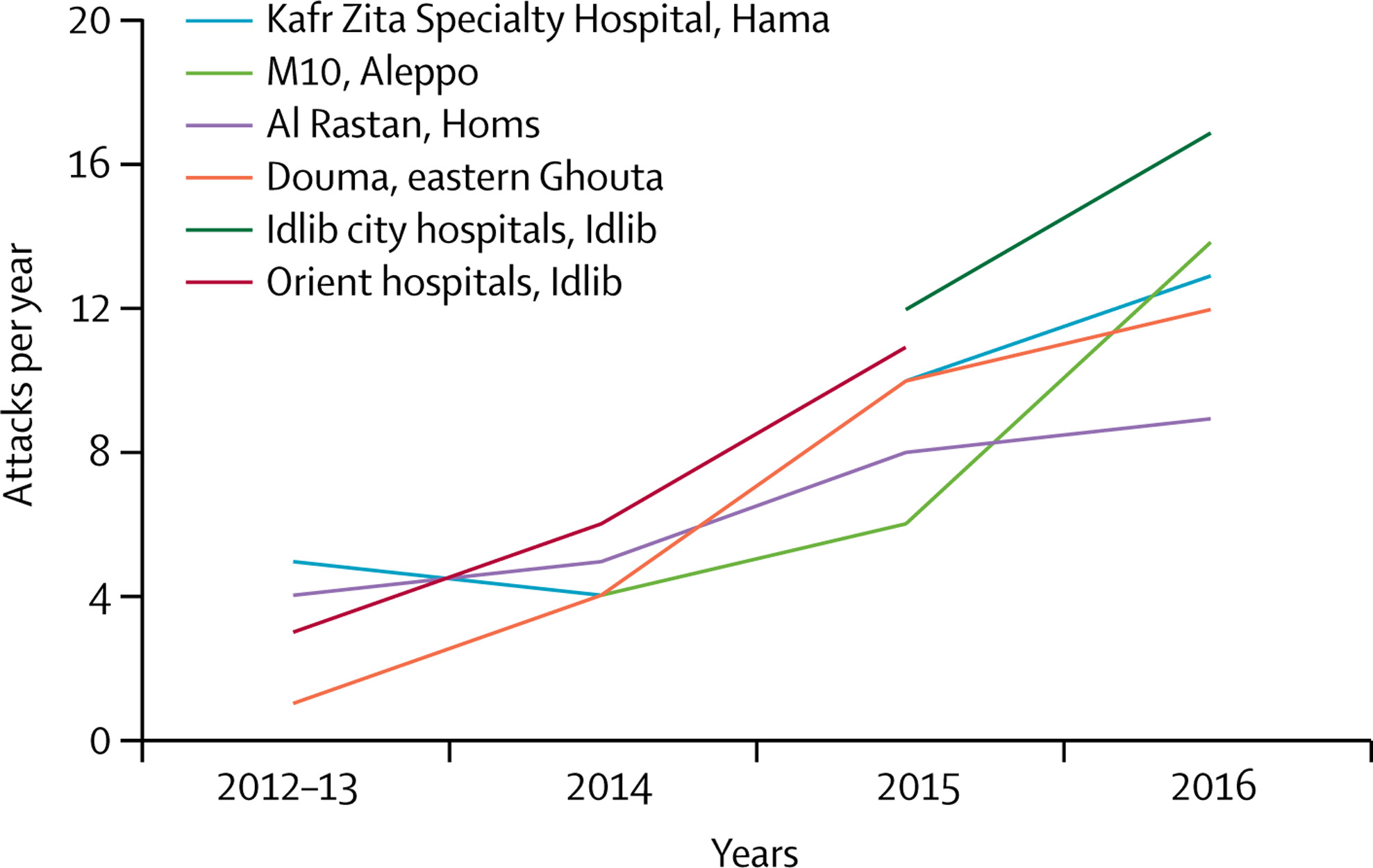
Attacks on hospitals – some of which I described in detail in a previous post – became not only more systematic but even repetitive, on a scale which the authors is wholly unprecedented.
‘Examination of attacks since 2012 on health facilities has revealed a distinct pattern of weaponisation.Analysis of attacks over several years in important opposition-held areas of Aleppo, Hama, Idlib, eastern Ghouta, and Homs reveals a pattern of repeated targeting with intention to shut access to health care, whether to impede opposition forces or to force civilian displacement.’
They list the effects of these attacks on healthcare in areas outside the control of the Syrian government – ‘rebel-held areas’ – but they also sketch the situation in areas under the control of the Islamic State:
Efforts to recruit foreign doctors through social media have reportedly helped IS to develop a functioning health system with modern facilities and equipment, qualified health workers, and a medical school in Raqqa where students train for free. But this health system is exclusive to IS, and foreign doctors are only permitted to provide care for IS members. For the rest of Raqqa’s civilians, over 1 million people, there are only 33 specialist doctors including just three obstetricians and one ophthalmologist, and just two public hospitals. Anecdotal reports indicate that health workers are forced to deliver care at gunpoint while others are arrested, abducted, or even executed for refusing to deliver care. To stop the exodus of health workers, IS uses the threat of seizure of homes and clinics in case of absence from work. Gender separation in these areas means that female health providers are subject to additional stress and restrictions, being forced to abide by IS dress code and to treat only female patients.
And for the benefit of the useful idiots inside the academy who deny these predations by the Syrian government on its own people, I should add that the report also discusses the situation inside government-controlled areas:
The bulk of Syria’s remaining health workers are in government-controlled areas, where there is variability in the capacity of health facilities and personnel. Workers from these areas have also reported challenges, but of a different nature to those working in non-government- controlled areas. Indiscriminate mortar attacks from rebel areas have adversely affected daily life and the public’s sense of security. Many health workers report facing multiple security checkpoints for their daily trip to a hospital or clinic. The collapsing economy has eroded living standards and restricted school and career options for offspring of health workers. Medical students fear the military draft and the risk of being sent to the battlefield. To avoid that fate, many seek whatever residency training positions are available upon graduation, irrespective of specialty. However, with the emigration of many experienced senior academics, fewer high-quality specialists are available to supervise the training of younger doctors. Travel restrictions due to sanctions and the need for leave permits from the government leave few choices for these doctors. Some doctors in these areas have indicated that the international media pay little attention to their plight. Others report being forced to breach ethical principles under unbearable pressure.
You can find an elaboration of these claims in personal testimonials here, which include this:
In November 2011, Dr. Zaki [a pseudonym], a military anaesthetist, was sent to Aleppo Military Hospital. This hospital usually received injured Syrian army combatants, but from the start of 2012, it began receiving civilian patients injured by pro-government forces during the peaceful demonstrations taking place in Idleb and Aleppo. Notably there was no conflict at this time in either city. These civilian patients were interrogated and tortured — either directly through electric shocks or beatings with rubber hoses, or indirectly, by leaving gunshot wounds or open fractures untreated,. A few days prior to the visit to the hospital by the UN-Arab League Special Envoy, who insisted on visiting all patients, Dr. Zaki was ordered by his superiors to find a way to keep these patients silent. The subtext of the order, issued by three generals, the first in charge of the hospital, the second, the head of military intelligence, and the third, head of the military secret police in Aleppo, was clear: “we know exactly who your family are and your wife’s family, and they will be arrested unless you comply” Under those conditions, Dr. Zaki used a combination of anaesthetic agents to sedate over 60 patients, so their wounds and shackles could literally be covered up, and no patient would be able to describe the torture and conditions of their confinement to the Special Envoy. Shortly after this, Dr. Zaki defected and fled to Turkey, along with his entire family and his wife’s family.
I urge you to read the whole report (it’s only 11 Lancet pages).
The report describes what it calls ‘siege medicine’, and for an update you can turn to another new report, this one from Physicians for Human Rights: Access Denied: UN aid deliveries to Syria’s besieged and hard-to-reach areas.
This is how it begins:
Death by infection because security forces do not allow antibiotics through checkpoints.
Death in childbirth because relentless bombing blocks access to clinics.
Death from diabetes and kidney disease because medicines to treat chronic illnesses ran out months ago.
Death from trauma because snipers stand between injured children and functioning hospitals.
And – everywhere – slow, painful death by starvation.
This is what one million besieged people – trapped mostly by their own government – face every day in Syria.
This is the unseen suffering – hidden under the shadow of barrel bombs and car bombs – that plagues the Syrian people as they enter a seventh grim year of conflict.
This is murder by siege.
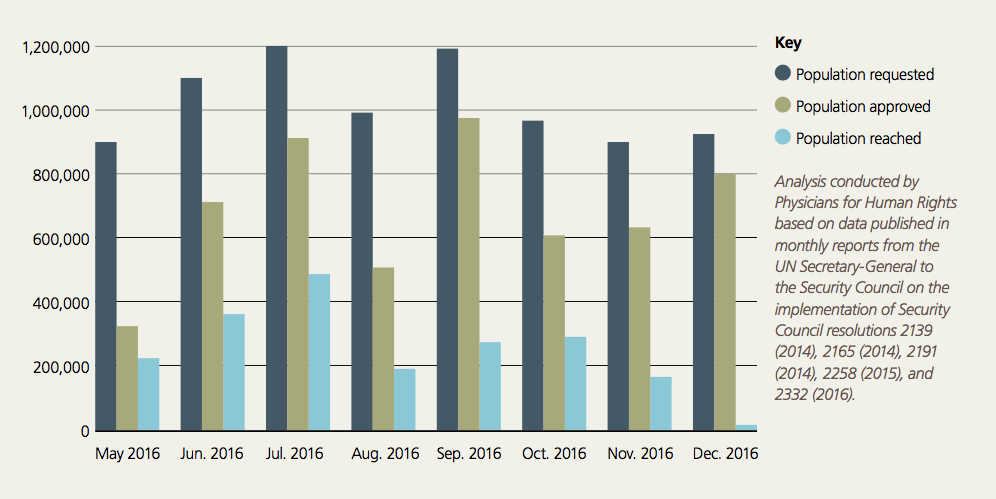
The report is limited to ‘the failure of the two-step approval process in ensuring the completion of UN interagency humanitarian convoys to besieged and hard-to-reach areas across Syria’; this excludes operations outside that approval process, but it still makes for remarkably grim reading. Here are the raw figures tabulating aid deliveries requested, approved and completed under the two-step process:
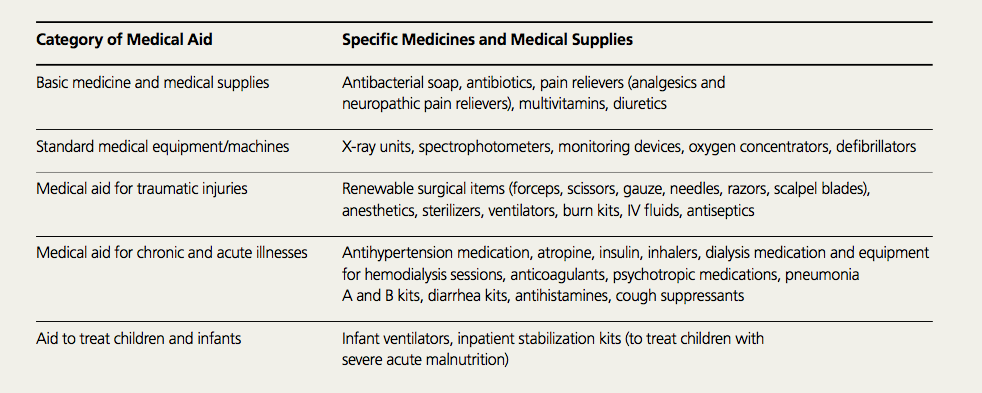
Even within these diminished envelopes there were further specific restrictions on medical supplies:
Throughout 2016, Syrian authorities specifically restricted medical aid to besieged and hard-to-reach areas, in direct violation of international humanitarian law.From February through December 2016, Syrian authorities prevented the delivery of more than 300,000 medical treatments to besieged and hard-to-reach areas.28 There is no clear definition of what constitutes a “medical treatment,” nor is there publicly available data on how much of each type of aid was removed from convoys. However, as [the examples in the tabulation below show], the disallowed medical aid included basic medicine, supplies, and equipment needed to treat traumatic, chronic, and acute conditions resulting from or aggravated by the sieges. In addition, it included medical aid speci cally meant to treat infants and children. Some of the disallowed medical aid could have been reused repeatedly to treat numerous people, thus its exclusion likely a ected large populations for prolonged periods of time.
In one particularly egregious example, Syrian government forces turned away an entire aid convoy as it was about to enter besieged Daraya in May 2016 because it contained medical aid and infant formula. Ironically, Syrian authorities in Damascus had limited the type of aid allowed on that convoy speci cally to medical aid, infant formula, and school supplies.