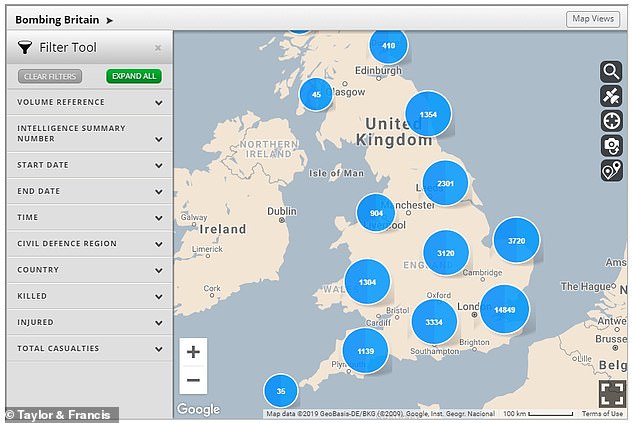
There is a stunning report (including an extended video) in today’s New York Times providing detailed evidence of Russian jets systematically attacking four hospitals in Syria in just twelve hours on 5/6 May 2019.
As regular readers will appreciate, this is a fraction of the total number of attacks on hospitals and clinics by Russian and Syrian aircraft – see my analysis in ‘Your turn, doctor’ here, ‘Death of the Clinic’ here and a stream of subsequent posts.
There have been other attempts to attribute culpability in the past – I’m thinking here of visual analysis by bellingcat and Forensic Architecture, for example – and, as the NYT notes, ‘recklessly or intentionally bombing hospitals is a war crime, but proving culpability amid a complex civil war is extremely difficult, and until now, Syrian medical workers and human rights groups lacked proof.’ What distinguishes this (brilliant) investigation is the incorporation of flights logs and intercepts of radio communications from the Russian Air Force that for the first time clearly and unambiguously show that these air strikes were deliberate, systematic and relentless attacks on known hospitals.
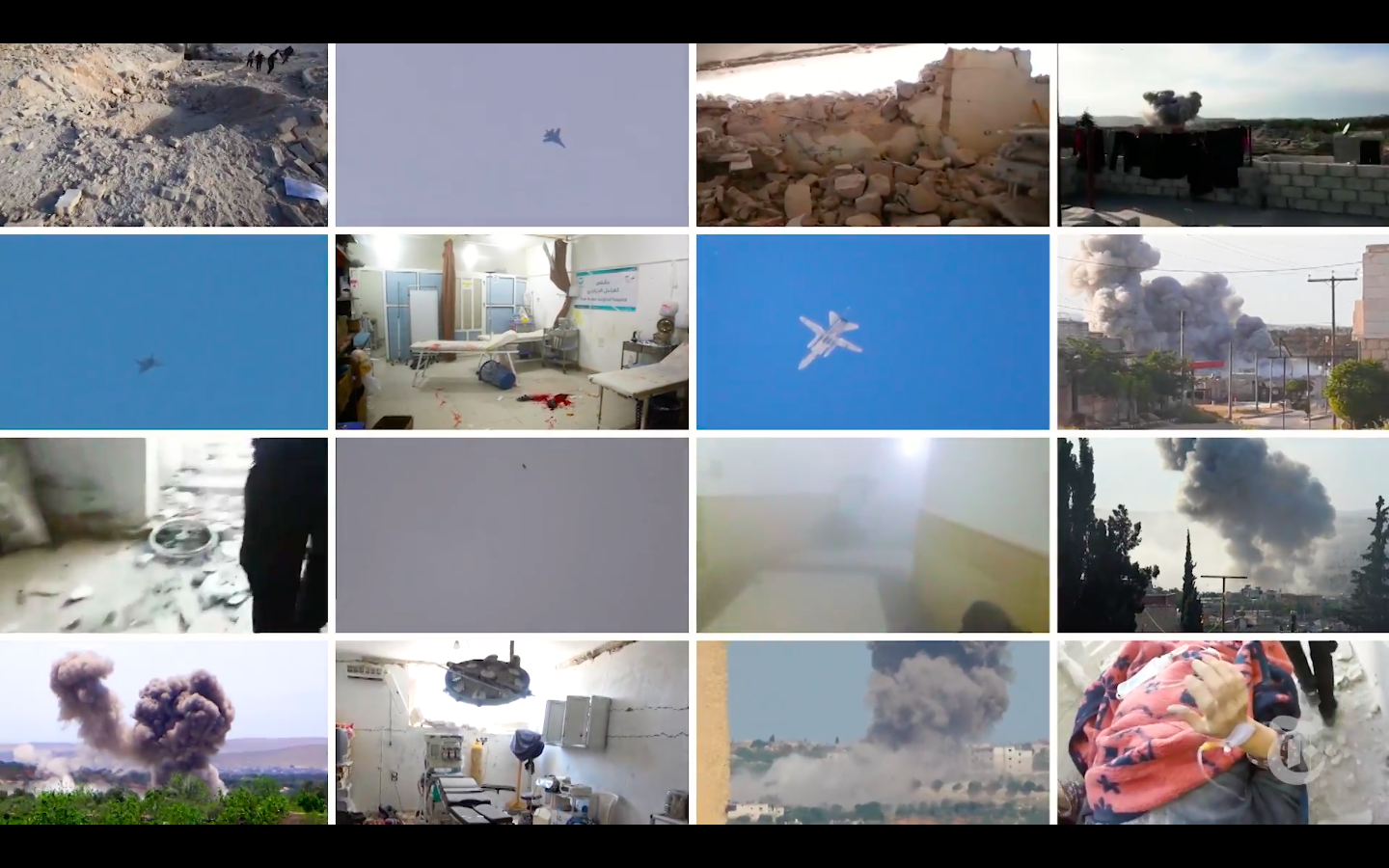
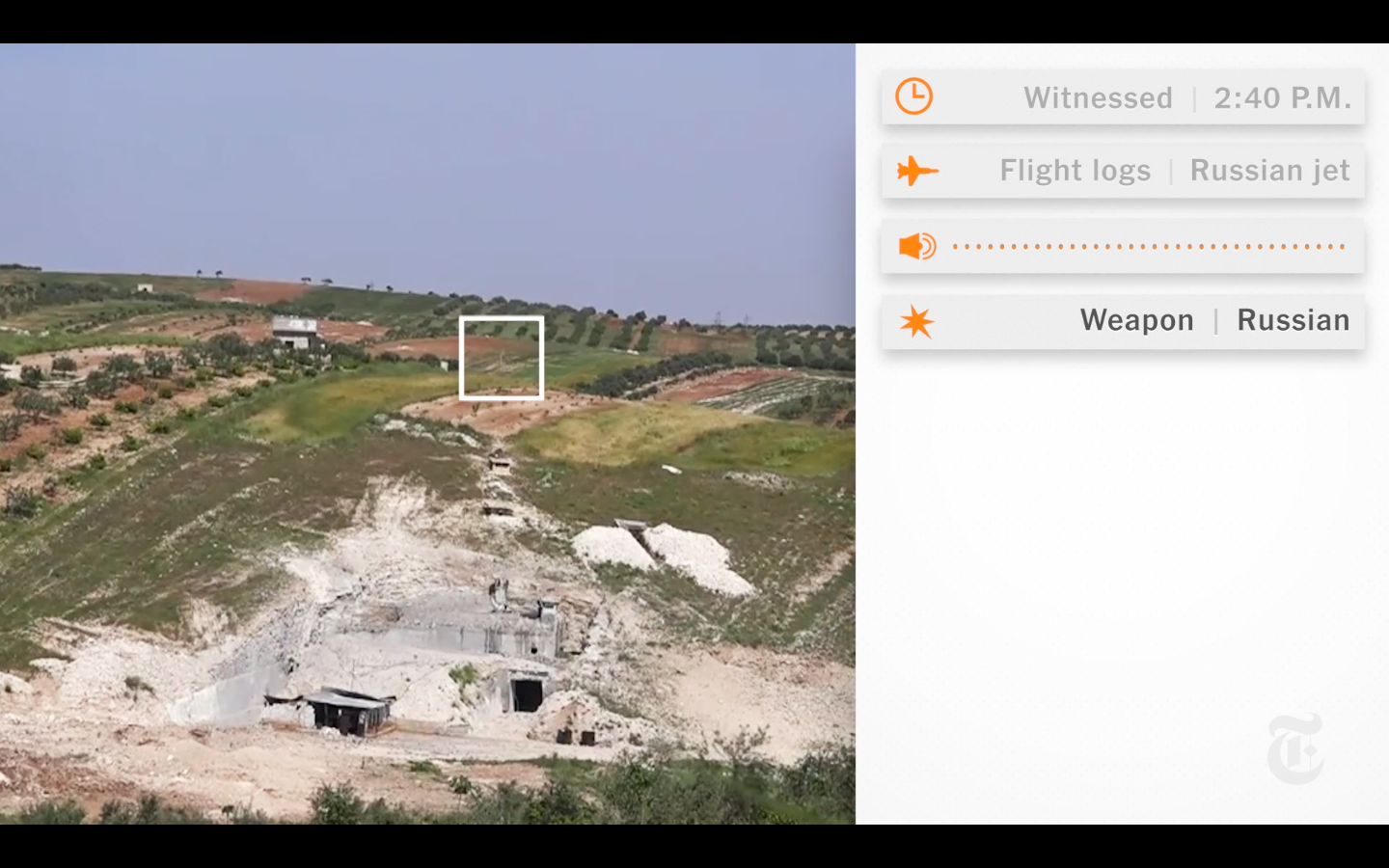
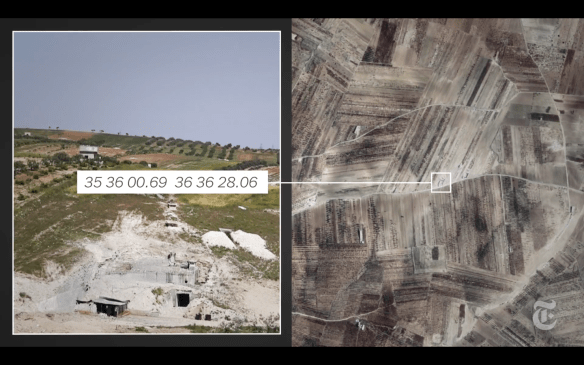
Here is the first attack analysed by the NYT; I’ve grabbed the images from the accompanying video..
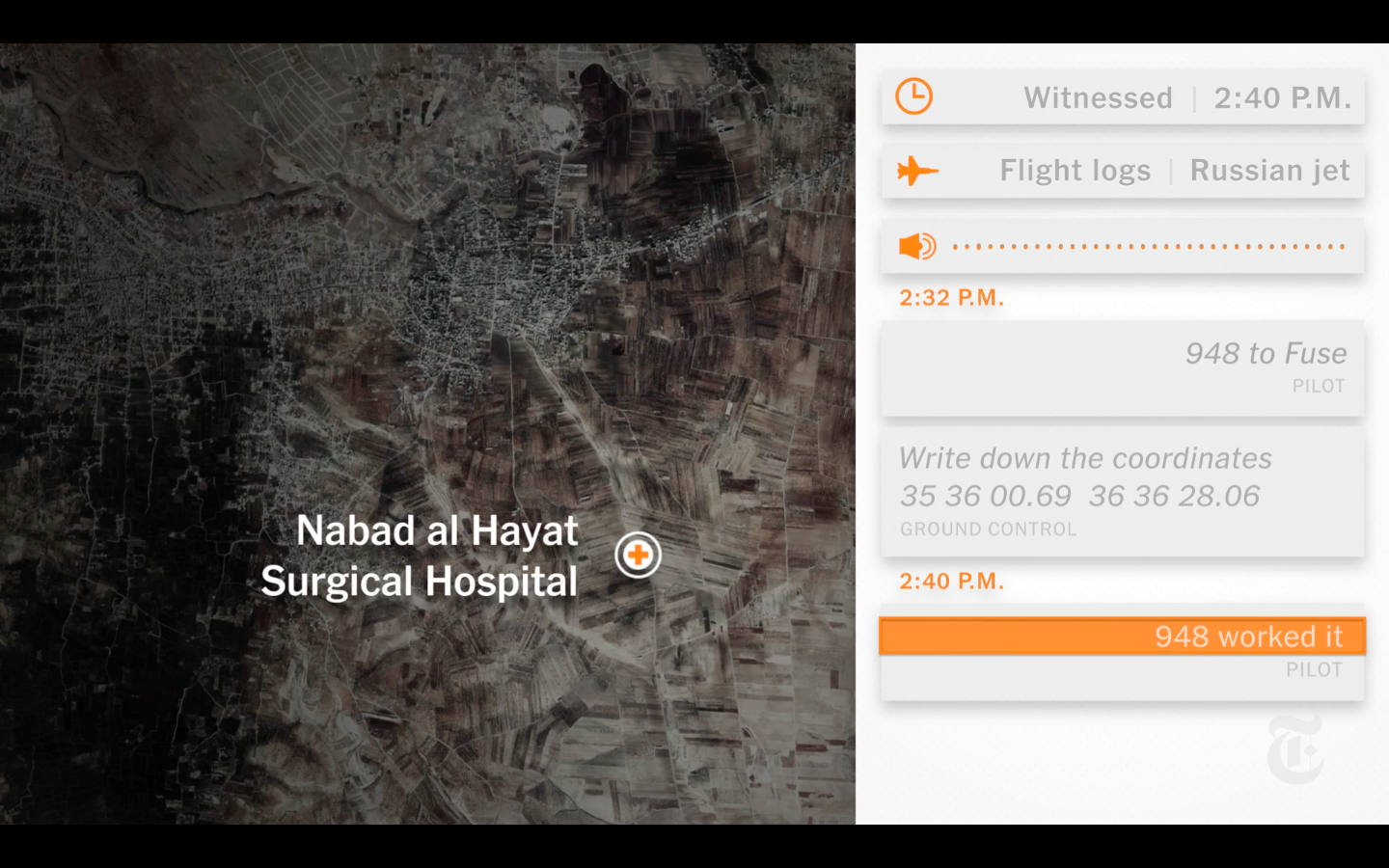
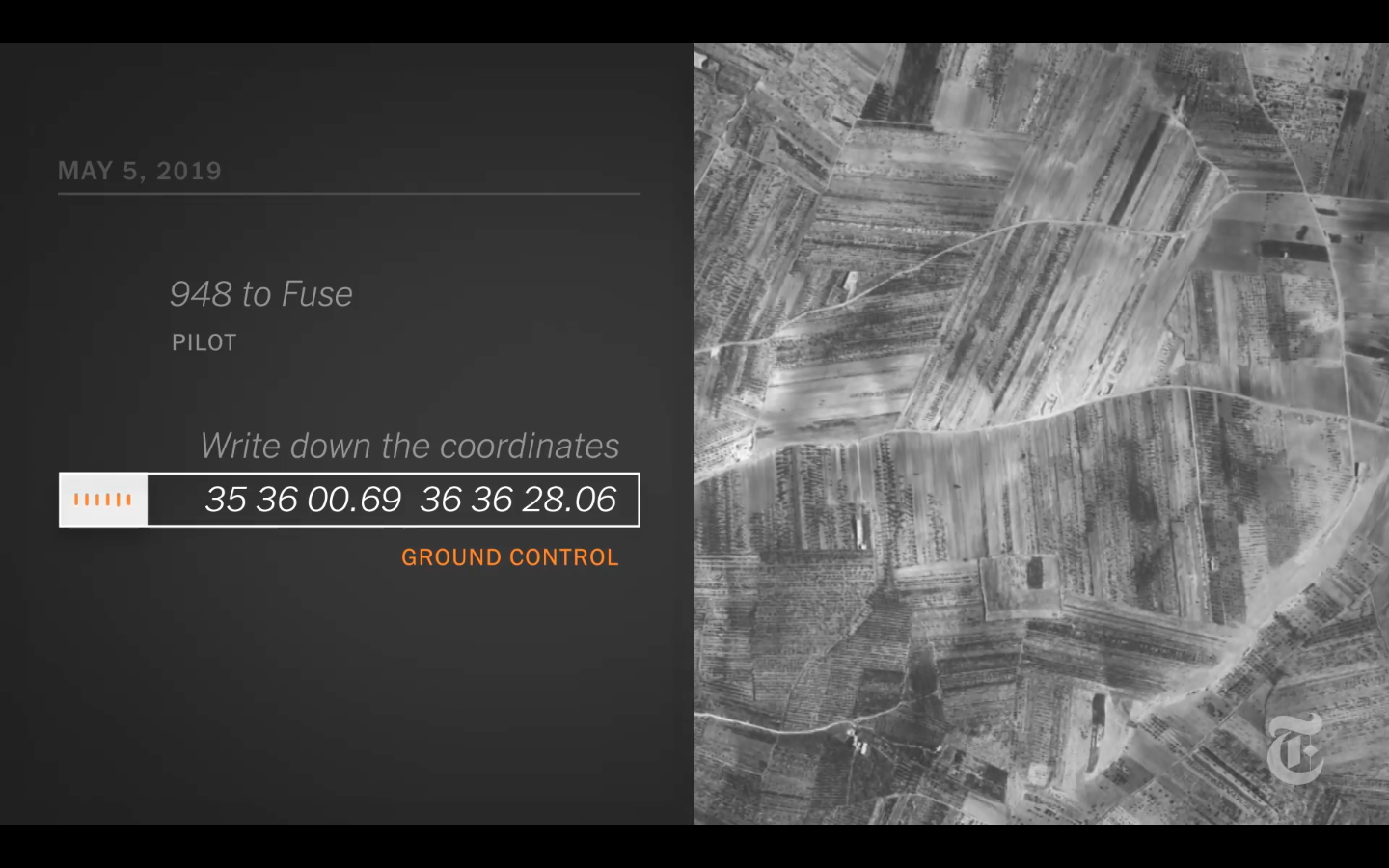
Nabad al Hayat had been attacked three times since it opened in 2013 and had recently relocated to an underground complex on agricultural land, hoping to be protected from airstrikes.
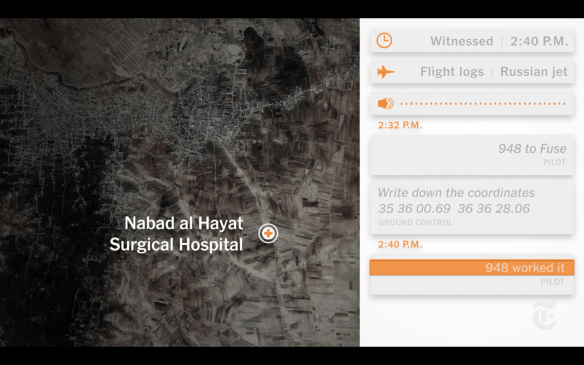
At 2:32 p.m. on May 5, a Russian ground control officer can be heard in an Air Force transmission providing a pilot with a longitude and latitude that correspond to Nabad al Hayat’s exact location.
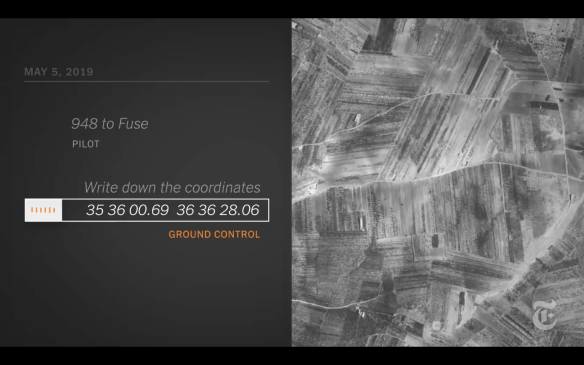
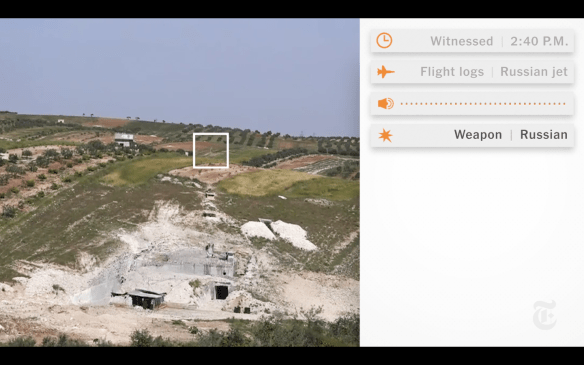
At 2:38 p.m., the pilot reports that he can see the target and has the “correction,” code for locking the target on a screen in his cockpit. Ground control responds with the green light for the strike, saying, “Three sevens.”
At the same moment, a flight spotter on the ground logs a Russian jet circling in the area.
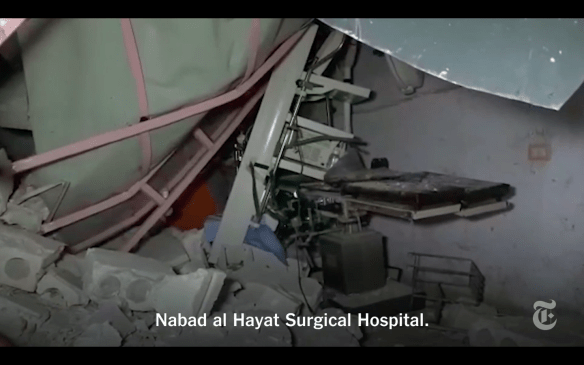
At 2:40 p.m., the same time the charity said that Nabad al Hayat was struck, the pilot confirms the release of his weapons, saying, “Worked it.” Seconds later, local journalists filming the hospital in anticipation of an attack record three precision bombs penetrating the roof of the hospital and blowing it out from the inside in geysers of dirt and concrete.

The staff of Nabad al Hayat had evacuated three days earlier after receiving warnings and anticipating a bombing [which is how journalists came to be on site to film the strike].
Another attack – detailed in the accompanying video – was on the Kafr Zita Cave Hospital (see also here).
As I’ve explained elsewhere, spaces of exception are not confined to the camp (as Agamben and others claim); war zones are also spaces in which particular groups of people are knowingly and deliberately exposed to death by removing the legal protections that would ordinarily safeguard them. But these are not legal ‘black holes’ either. The removal of those protections is itself (in part) the product of legal manoeuvers and, in the case of Syria, sleight of hand: Assad’s counterterrorism laws criminalised all medical aid to the opposition. That legal armature extends beyond domestic legislation: international humanitarian law and other quasi-legal formularies (including Rules of Engagement) are supposed to afford a modicum of protection to civilians. But throughout, hospitals and clinics are supposed to be ‘exceptions to the exception’: attacks on them, their staffs and patients are explicitly proscribed under IHL.
I’m bringing all these materials together – from attacks on hospitals on the coast of France and the Western Front in the First World War through Afghanistan (here and here) and Syria – in a major new essay: more soonest, though like most of my essays these days it threatens to metamorphose into a small book….
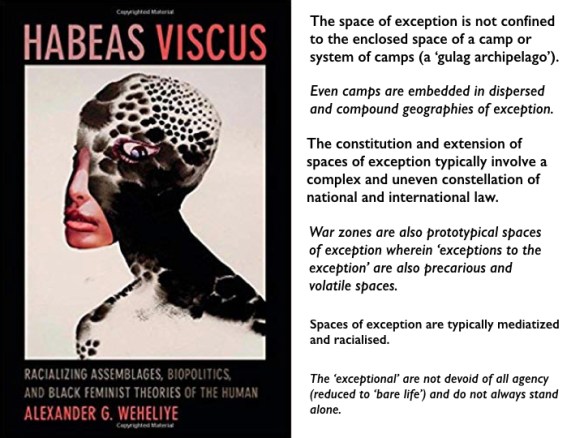
That essay will also elaborate the claims set out in the summary image above. One of the crucial points to sharpen, I think, is that the exception often appears earlier in time and distant in space from the enclosed contours of the camp or even the war zone that has replaced the traditional ‘battlefield’. I’m thinking here (in the case of the camp in the Second World War) on the systematic denigration of the Jews, the restrictions imposed on their life and movement in occupied cities, the roundups and detentions (see my lecture on occupied Paris under the TEACHING tab), their confinement to ghettoes: all of this in advance of their brutal transportation to the death camps hundreds of miles distant. If we don’t draw attention to those preliminary steps – if we fail even to recognise them – then it will be too late: the gates of the camp will clang shut.
What has this to do with hospital attacks? Quite simply: if the preliminary de-certification of hospitals and doctors in opposition-held areas is allowed to pass unchallenged, if we fail to contest the claim that these are ‘so-called hospitals’ and ‘so-called doctors’ (a familiar tactic of the Assad regime and its apologists), if we fail to respect medical neutrality, then the exception to the exception will vanish: hospital attacks will have been normalised.