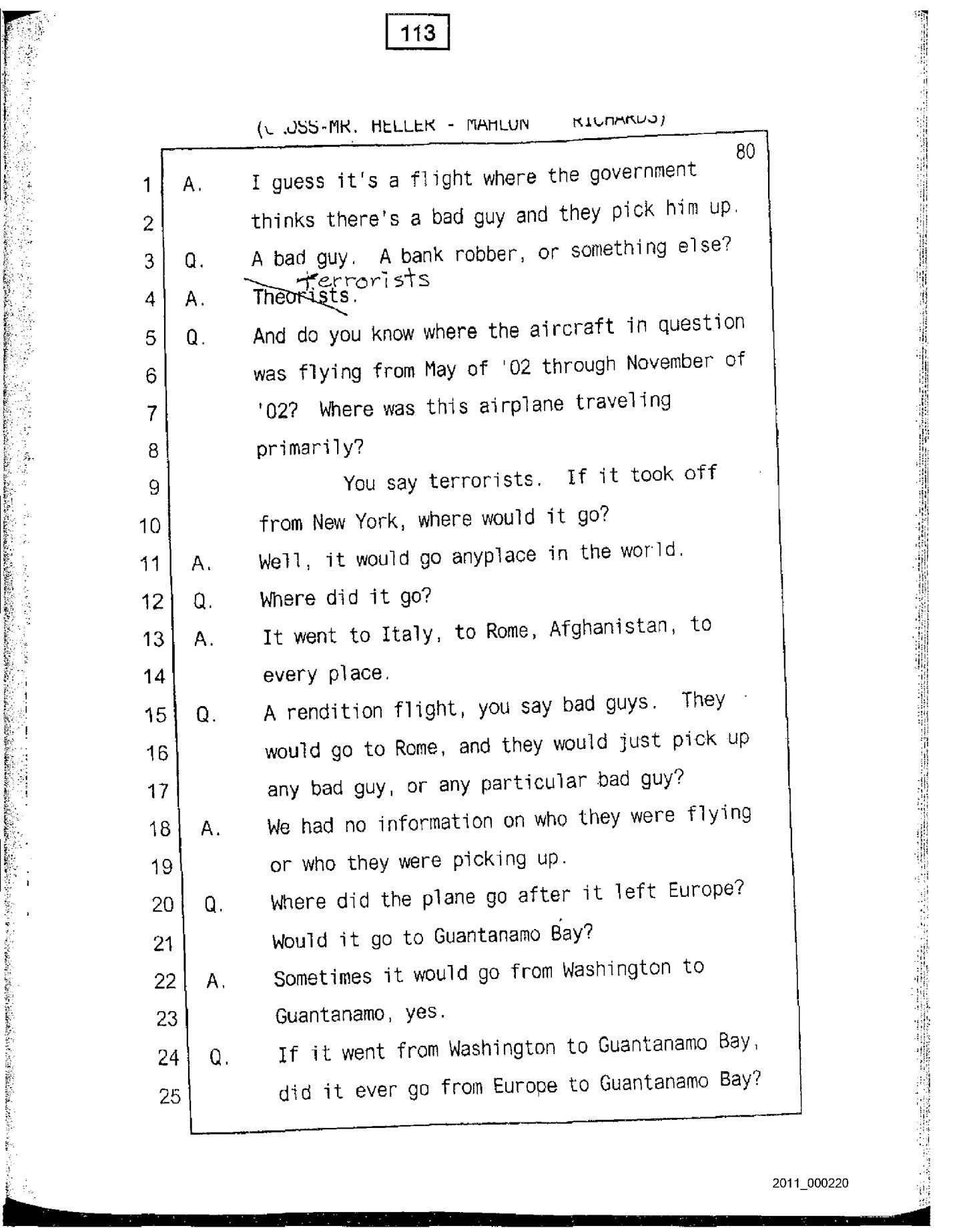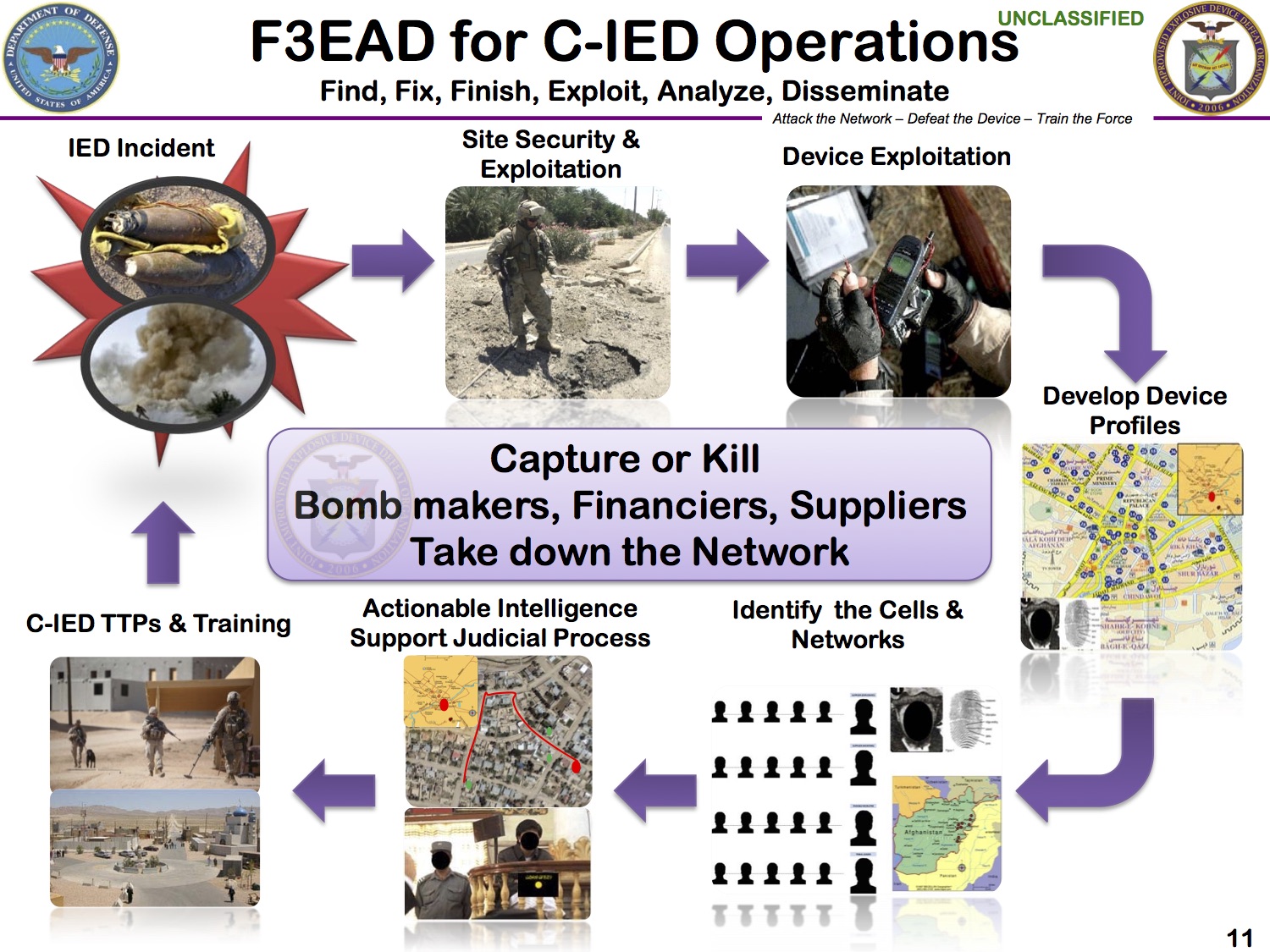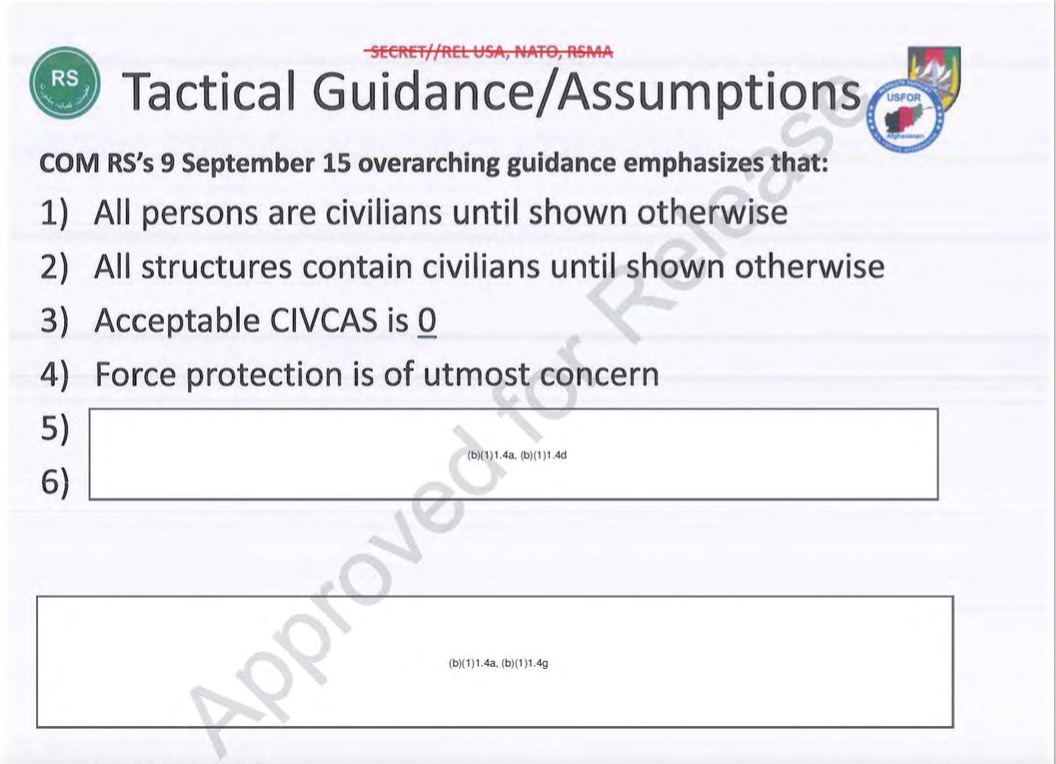
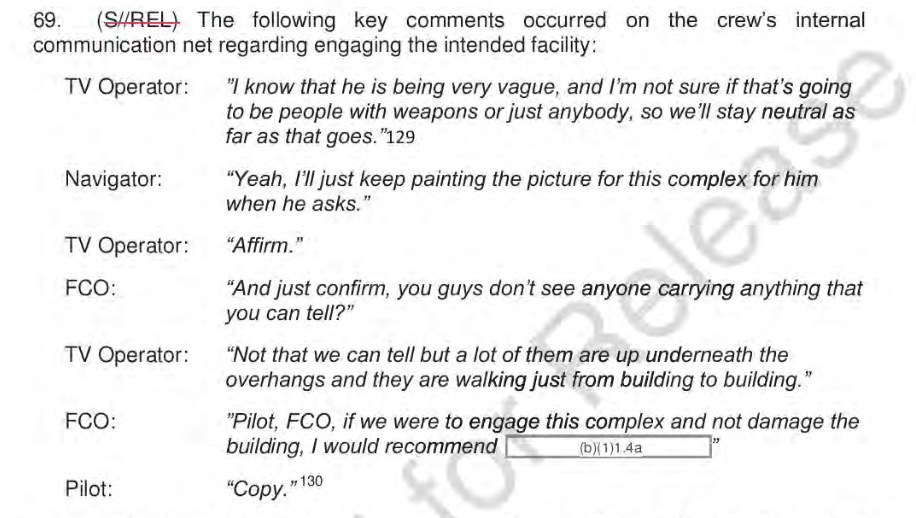
Finally US Central Command has released a redacted version of its investigation into the US airstrike on MSF’s Trauma Center in Kunduz (see my posts here, here and especially here). You can download it from CENTCOM’s Freedom of Information Act library here. (All the extracts pasted below capture communications exchanges before the attack, but the report includes redacted interviews with the participants involved in clearing, executing and continuing the air strike; the image above – and the title for this post – is taken from a briefing slide included in the report).
I’ll be spending the weekend reading it, but meanwhile the Intercept has published its own long-form account of the attack by May Jeong – ‘Death from the sky: searching for ground truth in the Kunduz hospital bombing‘. It was written before CENTCOM’s investigation was released but includes details from a series of interviews and is truly compelling reading.
I obviously won’t be alone in working my way through the report. Yesterday MSF was briefed by the head of CENTCOM, General Joseph Votel, and today released this preliminary statement:
MSF will take the time necessary to examine the U.S. report, and to determine whether or not the U.S. account answers the many questions that remain outstanding seven months after the attack.
MSF acknowledges the U.S. military’s efforts to conduct an investigation into the incident. Today, MSF and other medical care providers on the front lines of armed conflicts continually experience attacks on health facilities that go un-investigated by parties to the conflict. However, MSF has said consistently that it cannot be satisfied solely with a military investigation into the Kunduz attack. MSF’s request for an independent and impartial investigation by the International Humanitarian Fact Finding Commission has so far gone unanswered….
The hospital was fully functioning at the time of the airstrikes. The U.S. investigation acknowledges that there were no armed combatants within – and no fire from – the hospital compound.
The nature of the deadly bombing of the MSF Kunduz Trauma Centre, and the recurring attacks on medical facilities in Afghanistan, demand from all parties to the conflict a clear reaffirmation of the protected status of medical care in the country. MSF must obtain these necessary assurances in Afghanistan before making any decision on if it is safe to re-start medical activities in Kunduz.
The Pentagon has insisted that no war crimes were committed but confirmed that 16 people had been punished. Mark Thompson explains:
None of those involved will face court martial, but the administrative punishments levied against them—ranging from removal from command, letters of reprimand, to counseling—likely mark the end of their careers in uniform. None was identified by name. Those involved—the highest-ranking was a two-star general—included those aboard the AC-130 gunship that repeatedly fired on the Doctors Without Borders hospital in Kunduz, as well as members of the Army Special Force team on the ground that called in the strikes.
MSF has, understandably, condemned this response, arguing that the punishments
are out of proportion to the destruction of a protected medical facility, the deaths of 42 people, the wounding of dozens of others, and the total loss of vital medical services to hundreds of thousands of people. The lack of meaningful accountability sends a worrying signal to warring parties, and is unlikely to act as a deterrent against future violations of the rules of war.
That last sentence is particularly important, because there has been a steady increase in the targeting of medical personnel and medical facilities in Afghanistan, occupied Palestine, Syria and elsewhere: all gross violations of medical neutrality.
So this commentary from Joanne Liu (International President of MSF) and Peter Maurer (President of the International Committee of the Red Cross) – also published today – is much more than a response to the bombing of yet another MSF facility, this time in Aleppo:
What we are witnessing is a sustained assault on, and massive disregard for, the provision of healthcare during times of conflict. Under international humanitarian law and principles, health workers must be able to provide medical care to all sick and wounded regardless of political or other affiliation, whether they are a combatant or not. And under no circumstances should they be punished for providing medical care which is in line with medical ethics. The doctor of your enemy is not your enemy.
But we are confronted with violations of these fundamental rules, with serious humanitarian consequences, for entire communities and healthcare systems that are already stretched to the limit. And this is not just the opinion of MSF and the Red Cross Red Crescent Movement.
That is why we, as the presidents of MSF and the ICRC, welcome the proposal for a landmark UN resolution to protect healthcare. But we urge the UN security council to make the resolution effective. First, it should send a powerful political message that healthcare needs to be protected. All parties to an armed conflict must fully comply with their obligations under international law, including humanitarian law. And they must clearly state their respect for the delivery of impartial medical care during times of conflict.
Second, it must urge states and all parties to armed conflict to develop effective measures to prevent violence against medical personnel, facilities and means of transport. States need to bolster, where appropriate, their legislation including by lifting restrictions and sanctions impeding impartial wartime medical care.
Armed forces and all parties to a conflict should integrate practical measures for the protection of the wounded and sick and for those engaged in medical work. These should be incorporated into orders, rules of engagement, standard operating procedures and training.
Third, it must acknowledge that when attacks on medical facilities and personnel do take place, there needs to be full, prompt, impartial and independent investigations to establish the facts. It cannot only be the victims or perpetrators who attempt to establish the facts. And there should be regular and formal reporting of such attacks at the highest level and an annual debate in the security council.
Underpinning everything has to be the acceptance that the medical needs of people – no matter who they are, where they are from or what side they support or fight for – must take precedence. Medical staff are present in areas of conflict in order to care for the sick and wounded, on the basis of need. And only need. This is the fundamental principle of impartiality and is the basis of medical ethics. It is the very fact that doctors treat on the basis of need – and are not involved in hostilities – that they can claim protection under international humanitarian law.
But there is more. John Sifton from Human Rights Watch insists that General Viotel was simply wrong to claim that war crimes must be deliberate or intentional, so that those involved in the attacks on the MSF hospital could be absolved of criminal responsibility because the acts they committed were genuine mistakes. According to the New York Times, Sifton argued:
There are legal precedents for war crimes prosecutions based on acts that were committed with recklessness, and that recklessness or negligence do not necessarily absolve someone of criminal responsibility under the United States military code.