My main presentation at the AAG in Chicago was part of a session organised by Noam Leshem and Alasdair Pinkerton on Remnants of No Man’s Land: history, theory and excess (more on their larger project here). Here is an extended summary of what I had to say, together with some of my slides, but bear in mind that this all had to be done in 20 minutes so there wasn’t much room for nuance. Neither was there time to discuss civilian entanglements, both volunteers and victims, nor the sick: the presentation focuses on the wounded, even though the problems of trench foot, ‘trench flu’, and a host of other diseases were also extremely important. They do all receive attention in the larger project from which this is extracted. One last, geographical qualification: my discussion is limited to the evacuation of British and imperial troops from the Western Front.
My starting-point was the strange disappearance of the wounded from the field of battle. As John Keegan wrote in The Face of Battle, in most histories the ‘wounded apparently dematerialize as soon as they are struck down’; he was writing specifically about General Sir William Napier’s account of the battle of Albuera in 1811, but the point is a sharp one that can be enlisted as part of a more general critique of military history.
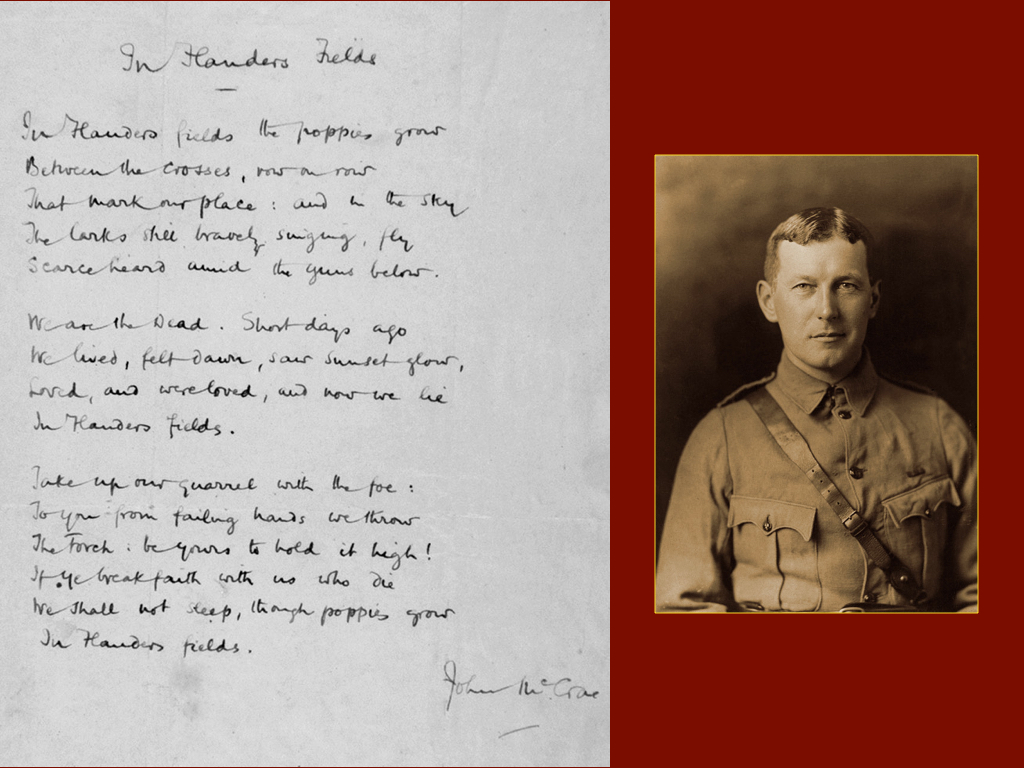
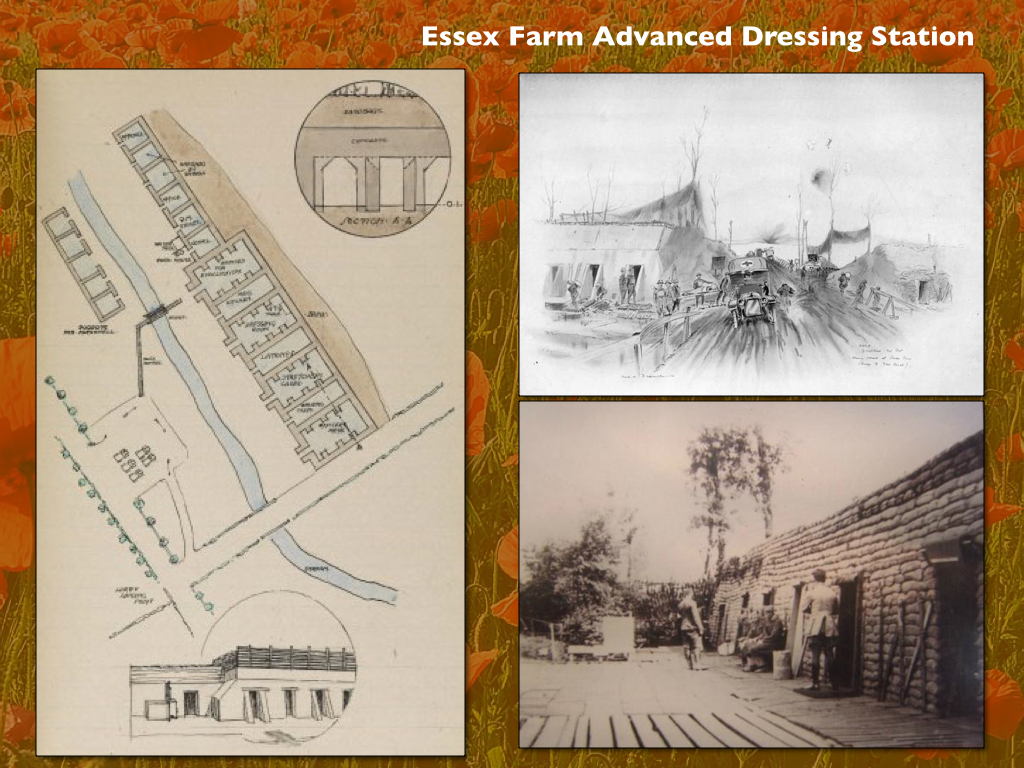
In the case of the First World War, the emphasis on those who lost their lives – on the dead not the wounded – derives not only from the sheer scale of the slaughter but also from the enduring landscape of memorialisation and commemoration. When John McCrae‘s elegaic poem ‘In Flanders Fields’ is recited every Remembrance Day – ‘In Flanders fields the poppies grow, between the crosses, row on row’ – it is all too easy to forget that he wrote those lines not only to commemorate the death of a close friend but that he did so at Essex Farm Advanced Dressing Station:


What lies behind those haunting lines – and that medical outpost – is a vast canvas of wounded men, which Christopher Nevinson captured as ‘The Harvest of Battle’ (below). The dead occupy the foreground, but behind them is the endless, moving panorama of the wounded whose precarious journeys took most of them far beyond ‘No Man’s Land’.

In fact, as Emily Mayhew reminds us, ‘being wounded was one of the most common experiences of the Great War’: on the Western Front, she writes, ‘almost every other British soldier could expect to become a casualty’.
But, perhaps not surprisingly, for the first six months of the war the British Expeditionary Force was unprepared for the scale of casualties, and even with the help of civilian volunteers and aid societies – Nevinson briefly served as a medical orderly with the Friends Ambulance Unit, for example – the remarkably long time it took to evacuate the wounded combined with the perilous nature of their improvised journeys to increase the mortality rate.

And so what Mark Harrison called the military-medical machine had to be speeded up – and moved closer to the field of battle.

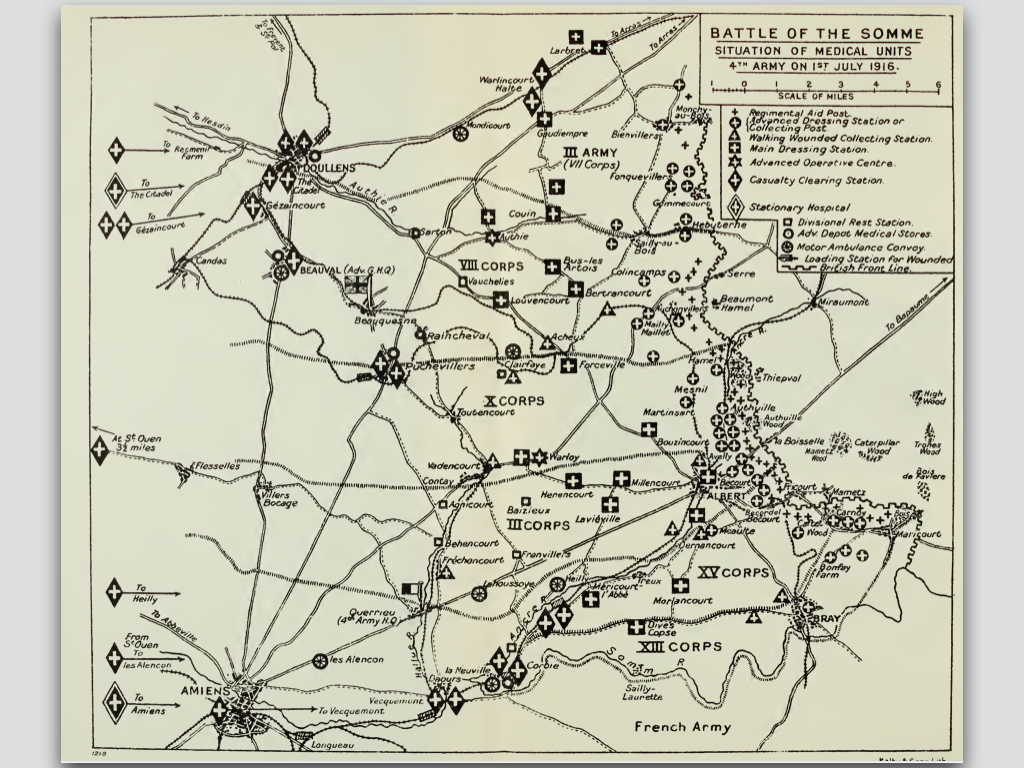
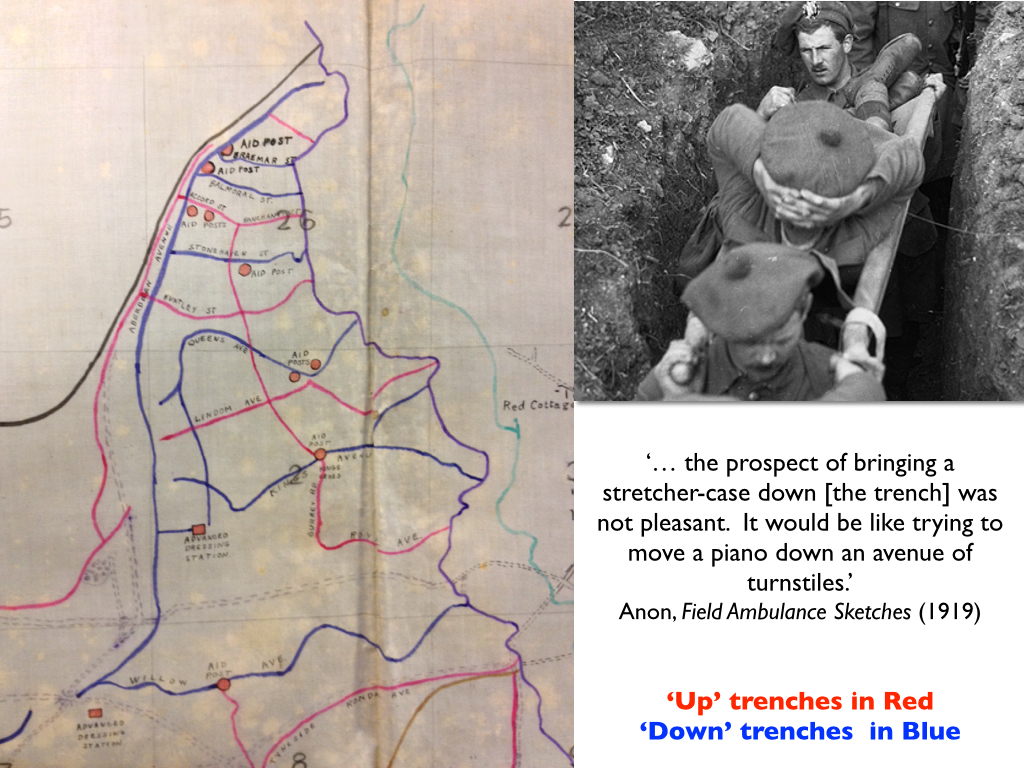
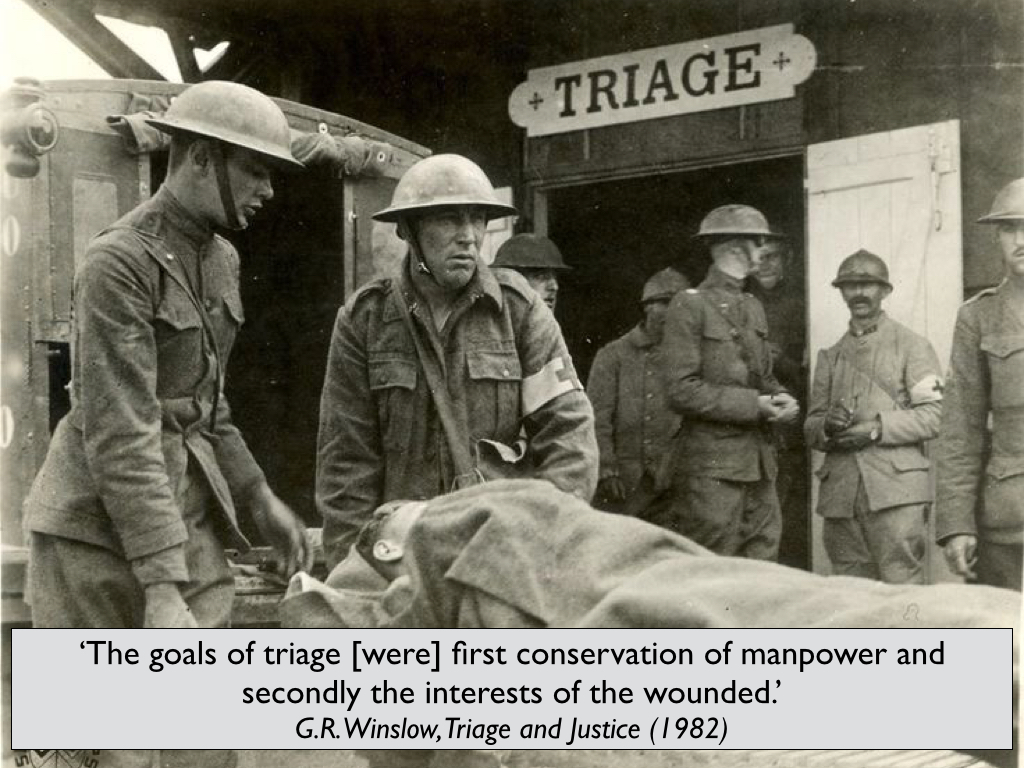
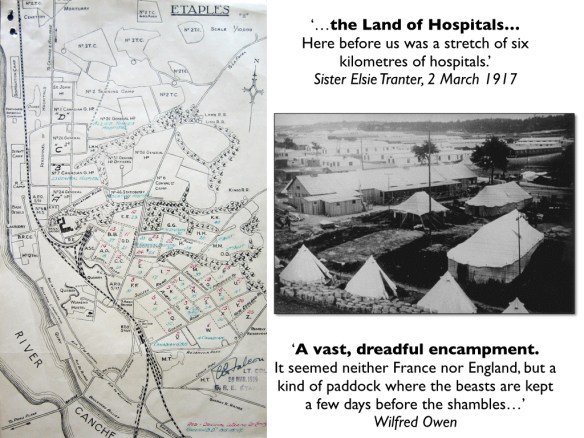
Before every major offensive elaborate plans for medical support were prepared: casualties were ‘cleared’ down the line as far and as fast as possible to make room for the newly injured, casualty clearing hospitals moved closer to the line, ambulances and stretcher-bearers made ready, and ‘down’ trenches designated for the efficient removal of the wounded (below).
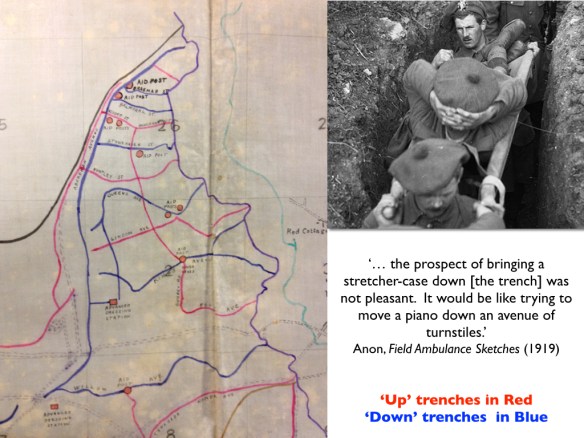
Soldiers wounded in ‘No Man’s Land’ – a term never recognised by the British General Staff, who insisted that they controlled the field of battle right up to the enemy front lines – were often immobilised and disoriented; some crawled into shell holes, seeking refuge below the field of fire, but it could take hours, even days before they were discovered and rescued (I’ll devote a later post to a detailed discussion of some of those cases).


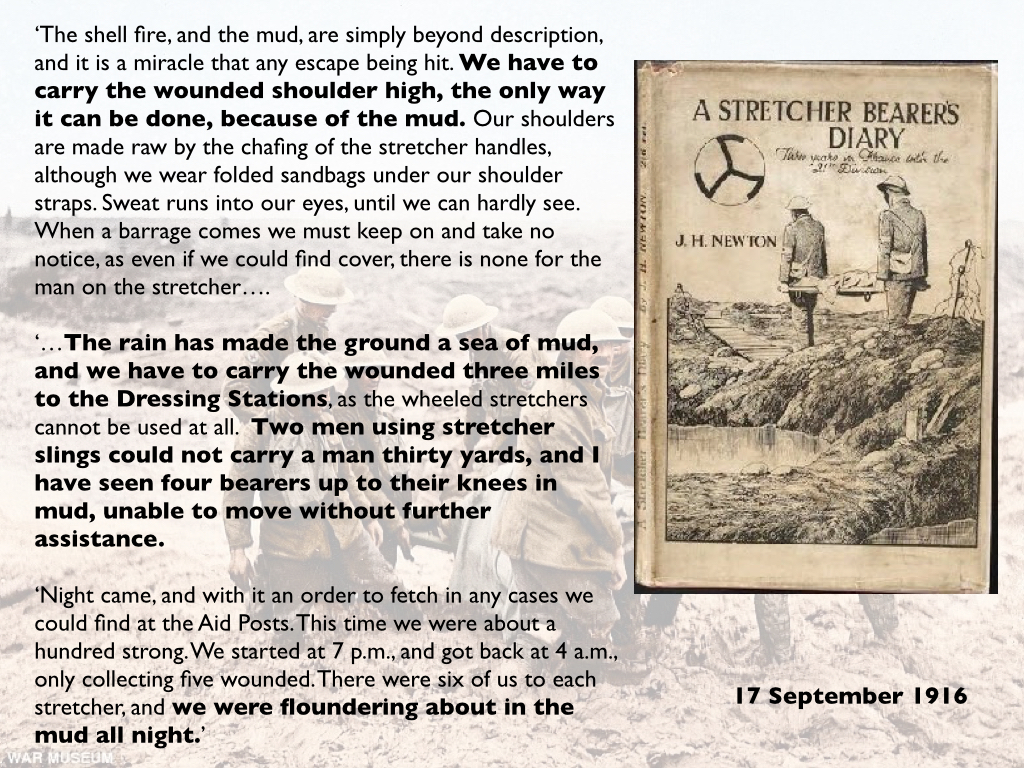
Sometimes their mates came to their rescue, sometimes the regimental stretcher bearers. But they too had to find their way through a dangerous and devastated terrain, often with no landmarks to guide them and on occasion made virtually impassable by the thick, cloying mud that was always – disconcertingly – much more than mud.

By now, they were in the care of the Royal Army Medical Corps’s Field Ambulance, and their first objective was an Advanced Dressing Station.
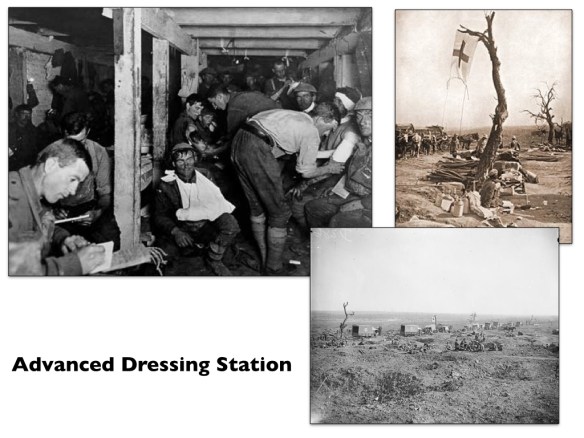

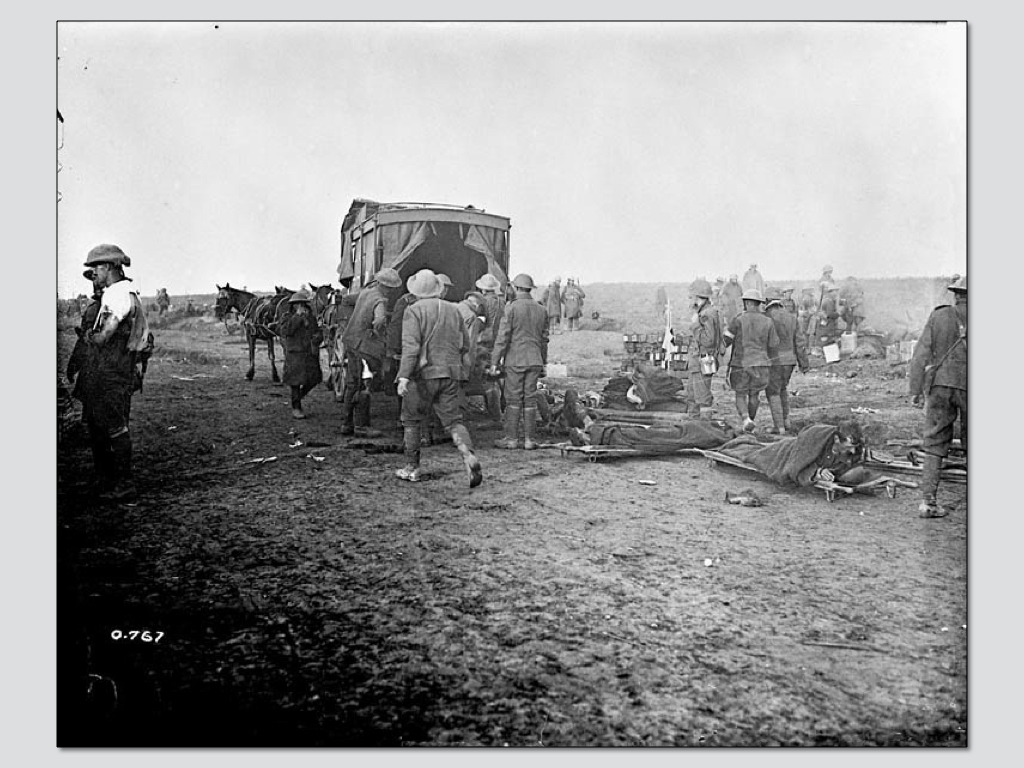
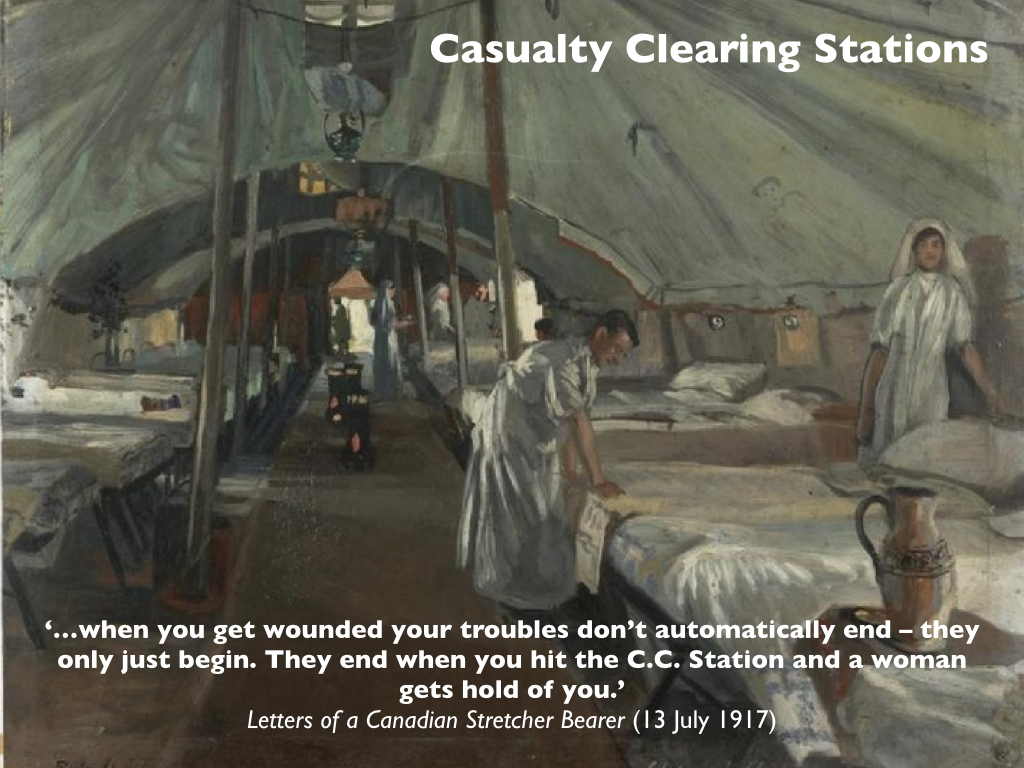
Those that needed anything beyond simple treatment or emergency surgery were sent on by horse or motor ambulance to a Casualty Clearing Station (a field hospital).

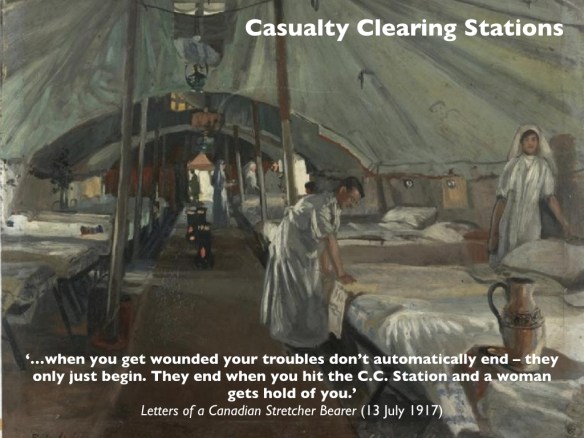
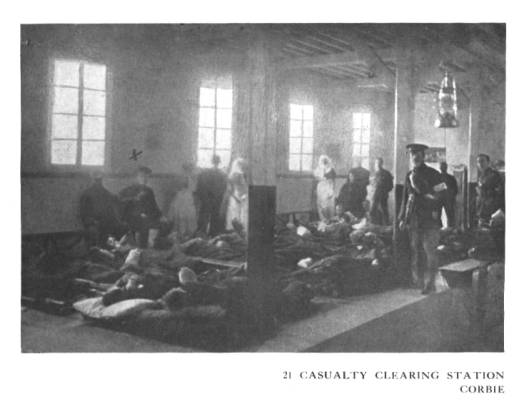
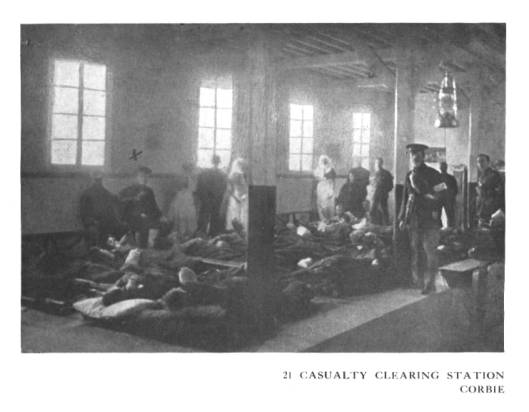
It was usually here that their first surgeries took place. The journalist Philip Gibb was shown around a CCS at Corbie and the experience haunted him for years:
After a visit there I had to wipe cold sweat from my forehead, and found myself trembling in a queer way. It was the medical officer—a colonel—who called it that name. “This is our Butcher’s Shop,” he said, cheerily. “Come and have a look at my cases. They’re the worst possible; stomach wounds, compound fractures, and all that. We lop off limbs here all day long, and all night. You’ve no idea!”
I had no idea, but I did not wish to see its reality. The M.O. could not understand my reluctance to see his show. He put it down to my desire to save his time—and explained that he was going the rounds and would take it as a favor if I would walk with him. I yielded weakly, and cursed myself for not taking to flight. Yet, I argued, what men are brave enough to suffer I ought to have the courage to see… I saw and sickened. These were the victims of “Victory” and the red fruit of war’s harvest-fields. A new batch of “cases” had just arrived. More were being brought in on stretchers. They were laid down in rows on the floor-boards. The colonel bent down to some of them and drew their blankets back, and now and then felt a man’s pulse. Most of them were unconscious, breathing with the hard snuffle of dying men. Their skin was already darkening to the death-tint, which is not white. They were all plastered with a gray clay and this mud on their faces was, in some cases, mixed with thick clots of blood, making a hard incrustation from scalp to chin. “That fellow won’t last long,” said the M. O., rising from a stretcher. “Hardly a heart-beat left in him. Sure to die on the operating-table if he gets as far as that… Step back against the wall a minute, will you?” We flattened ourselves against the passage wall while ambulance-men brought in a line of stretchers. No sound came from most of those bundles under the blankets, but from one came a long, agonizing wail, the cry of an animal in torture. “Come through the wards,” said the colonel. “They’re pretty bright, though we could do with more space and light.” In one long, narrow room there were about thirty beds, and in each bed lay a young British soldier, or part of a young British soldier. There was not much left of one of them. Both his legs had been amputated to the thigh, and both his arms to the shoulder-blades. “Remarkable man, that,” said the colonel. “Simply refuses to die. His vitality is so tremendous that it is putting up a terrific fight against mortality… There’s another case of the same kind; one leg gone and the other going, and one arm. Deliberate refusal to give in. ‘You’re not going to kill me, doctor,’ he said. ‘I’m going to stick it through.’ What spirit, eh?”…
“Bound to come off,” said the doctor as we passed to another bed. “Gas gangrene. That’s the thing that does us down.” In bed after bed I saw men of ours, very young men, who had been lopped of limbs a few hours ago or a few minutes, some of them unconscious, some of them strangely and terribly conscious, with a look in their eyes as though staring at the death which sat near to them, and edged nearer. “Yes,” said the M. O., “they look bad, some of ’em, but youth is on their side. I dare say seventy-five per cent. will get through. If it wasn’t for gas gangrene—“
He jerked his head to a boy sitting up in bed, smiling at the nurse who felt his pulse. “Looks fairly fit after the knife, doesn’t he? But we shall have to cut higher up. The gas again. I’m afraid he’ll be dead before to-morrow. Come into the operating-theater. It’s very well equipped.”
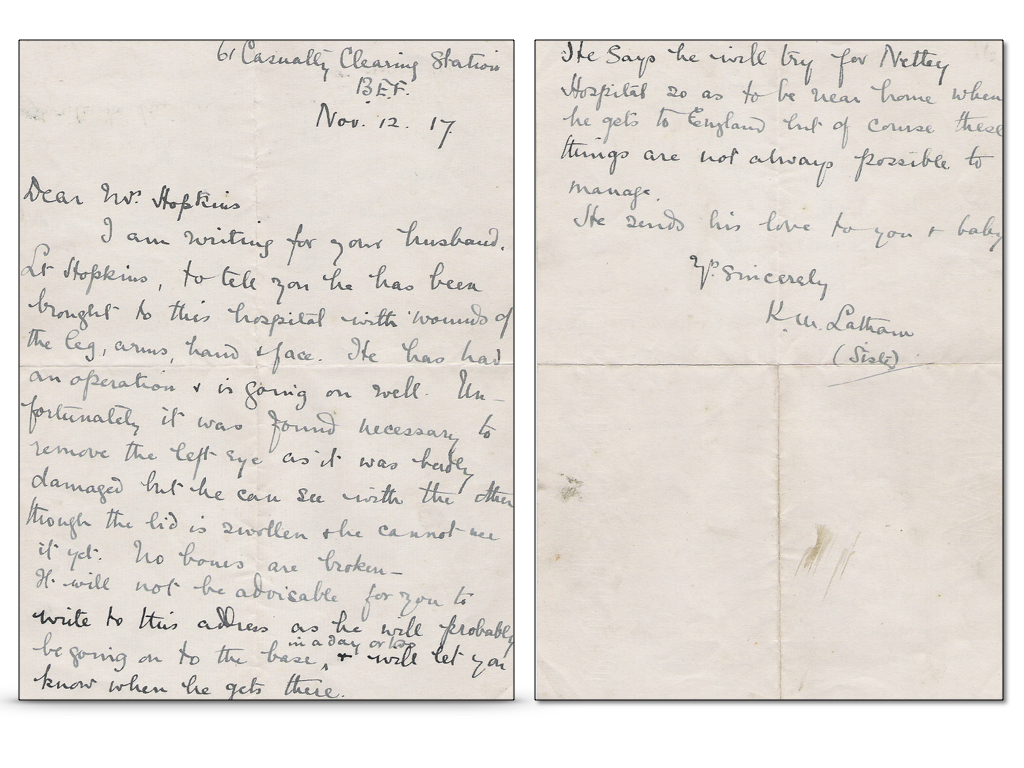
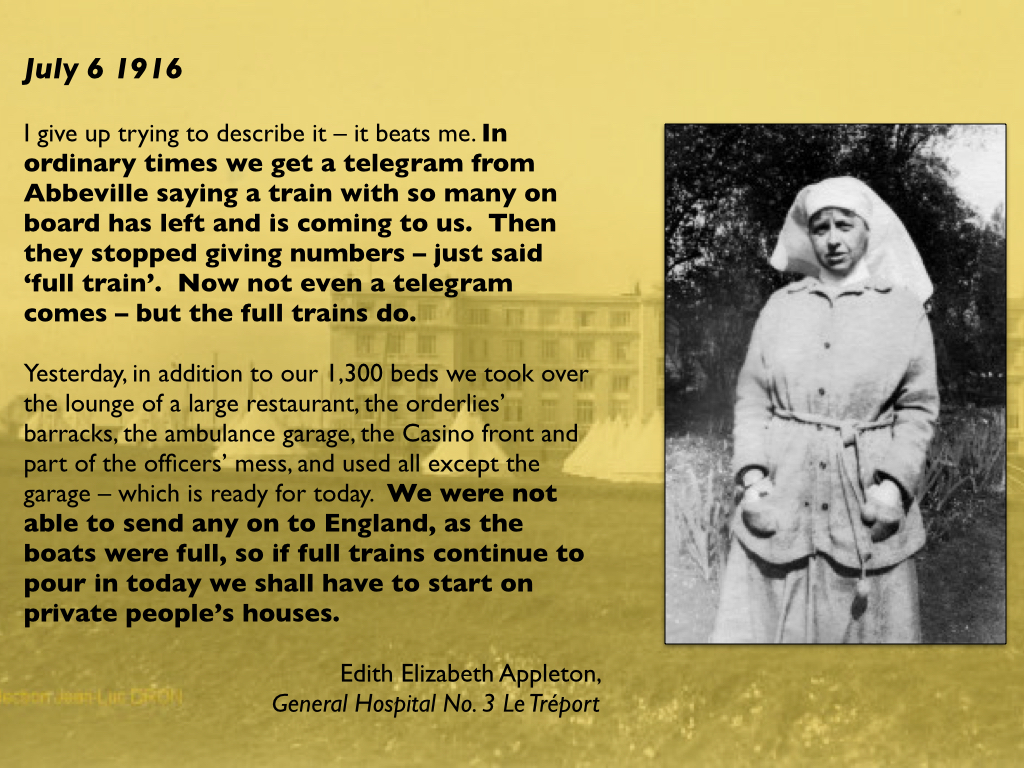
By now the bureaucratic machine had been activated: labels had been attached to the wounded and field medical cards (‘tickets’) completed; telegrams had been sent to advise families, and nurses had often written letters home on their patients’ behalf.


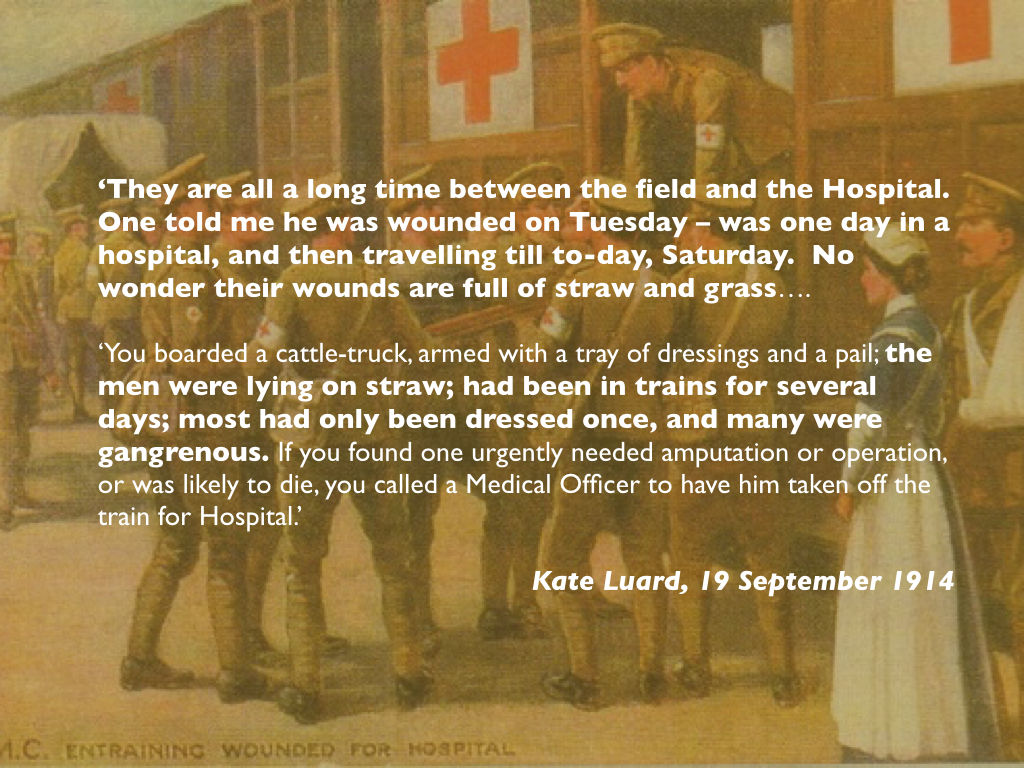
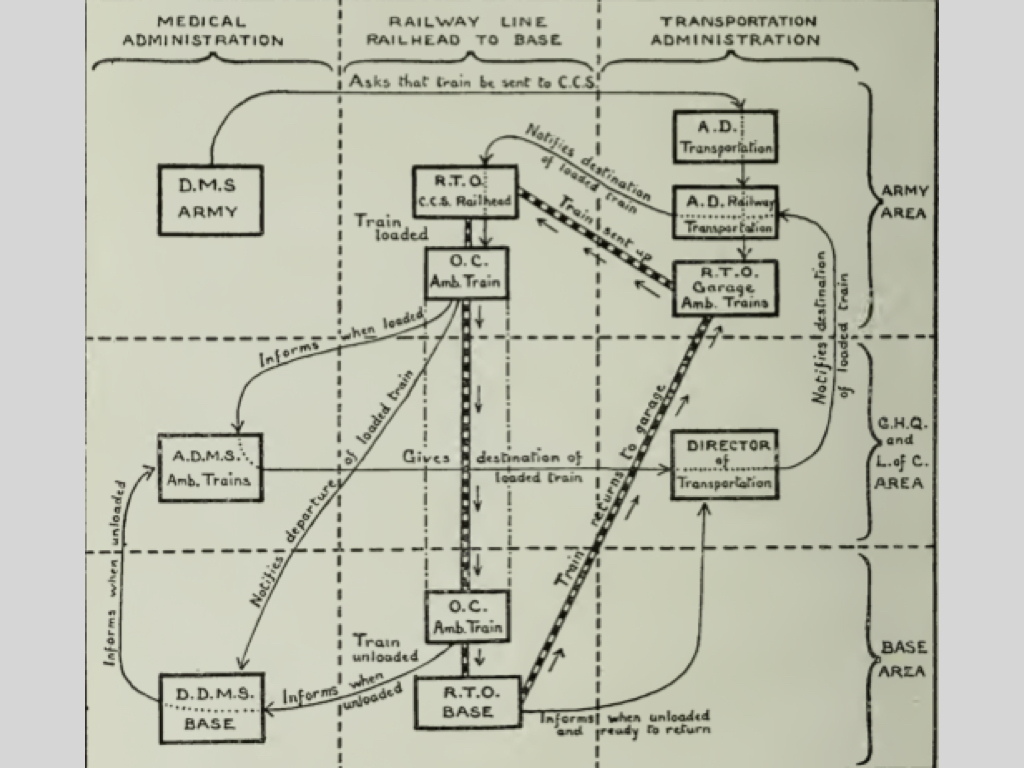
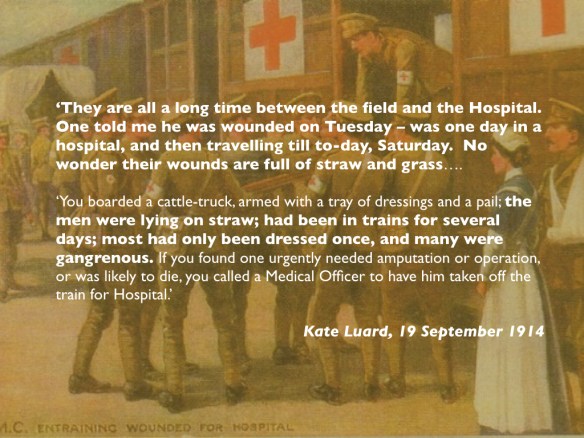
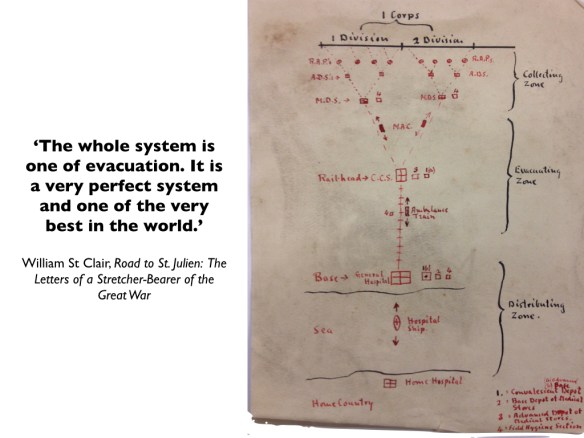
The next stage for the most seriously wounded was evacuation by ambulance train to a base hospital on the French coast. There was a considerable bureaucracy involved in planning these movements, but for all the neatness and symmetry of the organisational diagrams – part of Clausewitz‘s ‘paper war’ – there were all sorts of delays.


Priority was given to trains rushing reinforcements, supplies and ammunition to the front, and ambulance trains were frequently marooned in sidings waiting for them to pass so that journeys that might have taken hours could take days. It was not uncommon for an ambulance train to arrive at a base hospital to find that there was little or no room for new patients and all but the most grievous cases had to travel on to the next.

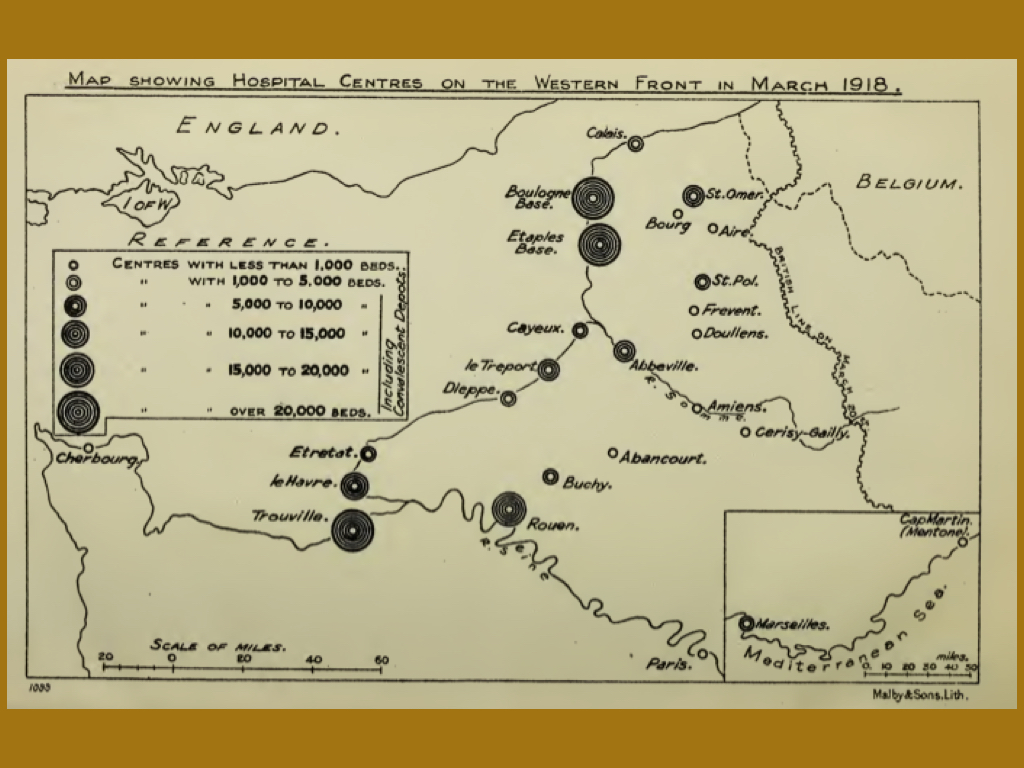
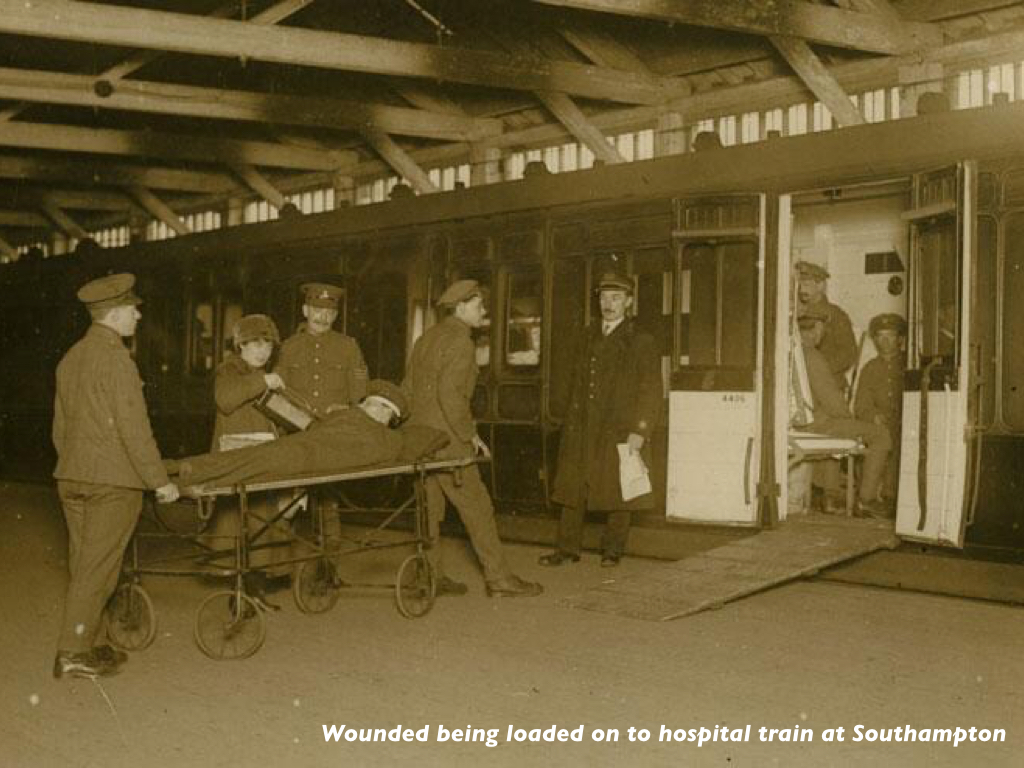
Many patients were treated at the base hospitals, but those with more serious wounds were evacuated by hospital ship to Britain. This stage of the journey was no less dangerous than the previous one: as the war continued, there was an increasing danger of mines and submarines in the Channel.


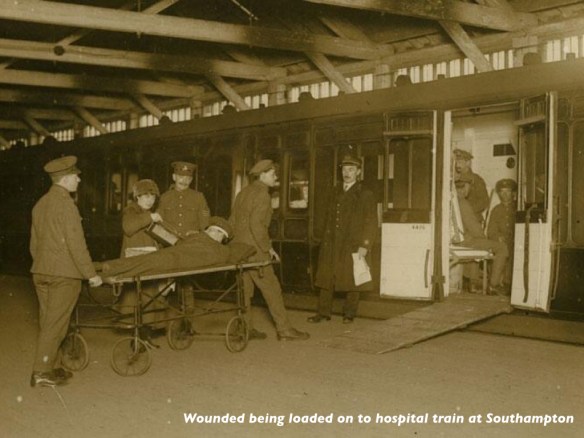
A distinctive geography of the wounded emerged. If they arrived at Southampton, the most critical cases were taken by train straight to the Royal Victoria Military Hospital at Netley, which treated as many as 50,000 patients during the war. According to Lyn McDonald,
‘Those who could not be accommodated, and those who were seriously wounded but likely to survive a longer journey, were sent on by train to Birmingham, Bristol, Exeter, Leicester, Norwich and Plymouth. But seven out of every ten hospital trains were directed to London, and during the first days of the Somme they rolled in almost every hour to Charing Cross and Paddington stations.’


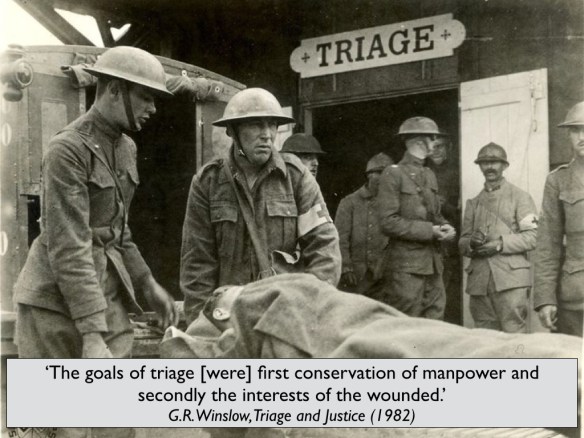
This is, of course, a highly abbreviated account of the casualty evacuation chain, and in the larger project from which this is derived I provide many more details. But I think I’ve said enough to show that the chain was, in effect, a production line with an elaborate division of labour (again, in the larger study I show how class – or more accurately, rank – gender and race segmented the chain in various ways). Indeed, in The Politics of Wounds Ana Carden-Coyne argues that what she calls ‘the Taylorist approach in modern war’ – and remember that this was industrial war on the grand (guignol) scale – ‘was particularly evident in the assembly-line style of evacuation and triage.’
This prompts two concluding observations.
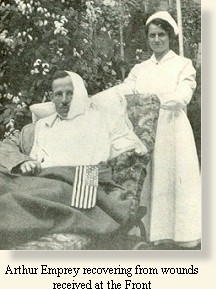
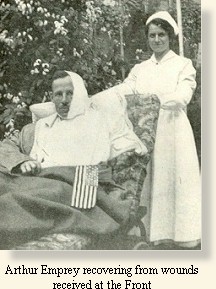
First, what was the instrumental logic that animated the evacuation chain? After all, it was an expensive undertaking, as Arthur Empey (himself wounded on the Western Front) realised in this re-calculation of the chain:
It may sound heartless and inhuman, but it is a fact, nevertheless, that from a military stand-point it is better for a man to be killed than wounded.
 If a man is killed he is buried, and the responsibility of the government ceases, excepting for the fact that his people receive a pension. But if a man is wounded it takes three men from the firing line, the wounded man and two men to carry him to the rear to the advanced first-aid post. Here he is attended by a doctor, perhaps assisted by two R.A.M.C. men. Then he is put into a motor ambulance, manned by a crew of two or three. At the field hospital, where he generally goes under an anaesthetic, either to have his wounds cleaned or to be operated on, he requires the services of about three to five persons. From this point another ambulance ride impresses more men in his service, and then at the ambulance train, another corps of doctors, R.A.M.C. men, Red Cross nurses, and the train’s crew. From the train he enters the base hospital or Casualty Clearing Station, where a good-sized corps of doctors, nurses, etc., are kept busy. Another ambulance journey is next in order — this time to the hospital ship. He crosses the Channel, arrives in Blighty — more ambulances and perhaps a ride for five hours on an English Red Cross train with its crew of Red Cross workers, and at last he reaches the hospital. Generally he stays from two to six months, or longer, in this hospital. From here he is sent to a convalescent home for six weeks.
If a man is killed he is buried, and the responsibility of the government ceases, excepting for the fact that his people receive a pension. But if a man is wounded it takes three men from the firing line, the wounded man and two men to carry him to the rear to the advanced first-aid post. Here he is attended by a doctor, perhaps assisted by two R.A.M.C. men. Then he is put into a motor ambulance, manned by a crew of two or three. At the field hospital, where he generally goes under an anaesthetic, either to have his wounds cleaned or to be operated on, he requires the services of about three to five persons. From this point another ambulance ride impresses more men in his service, and then at the ambulance train, another corps of doctors, R.A.M.C. men, Red Cross nurses, and the train’s crew. From the train he enters the base hospital or Casualty Clearing Station, where a good-sized corps of doctors, nurses, etc., are kept busy. Another ambulance journey is next in order — this time to the hospital ship. He crosses the Channel, arrives in Blighty — more ambulances and perhaps a ride for five hours on an English Red Cross train with its crew of Red Cross workers, and at last he reaches the hospital. Generally he stays from two to six months, or longer, in this hospital. From here he is sent to a convalescent home for six weeks.
If by wounds he is unfitted for further service, he is discharged, given a pension, or committed to a Soldiers’ Home for the rest of his life, — and still the expense piles up. When you realize that all the ambulances, trains, and ships, not to mention the man-power, used in transporting a wounded man, could be used for supplies, ammunition, and reinforcements for the troops at the front, it will not appear strange that from a strictly military standpoint, a dead man is sometimes better than a live one (if wounded).
Hence, for example, the orders recorded by A.M. Burrage:
The instructions given to stretcher-bearers are rather harsh. “ If you find two men wounded, and can take only one away, take away the one more likely to make a fit soldier again.” Therefore the one more urgently in need of attention must be left to die, because he would walk with a limp and would never again be able to carry a pack. Sound business, of course, but just a little hard.
Kate Luard captured another dimension of this when she wrote in January 1915:
‘The ambulance trains do so much bringing the British Army from the field that I hope some other trains are busy bringing the British Army to the field, or there can’t be many left in the field…’
And Emily Mayhew provides this bleak vignette from a medical orderly that captures the seemingly insatiable drive of industrial war:
An ordinary train, similar to the one that had brought him to the front, was at one end unloading reinforcements, while at the other end it was filling up with wounded men.
The logic, then, was one of ‘salvage’; four out of every five men wounded on the Western Front were returned to the fighting, which was the over-riding objective of the military-medical machine.
Second, the division of labour was also a division of life: the dead from the wounded, the dying from the ‘salvageable’, and the wounded from the unwounded or yet-to-be-wounded. The last was not the least. For breaching that separation could have the most unsettling consequences of all:

***
What started me on this journey was Emily Mayhew‘s brilliantly conceived Wounded and an excellent series of articles by Martin Bricknell in the Journal of the Royal Army Medical Corps: see in particular here.
You can also find more on the casualty evacuation chain from the Western Front at Beyond the Trenches here and here, the Long, Long Trail here, the Medical Front here, and the Royal Army Medical Corps site here.
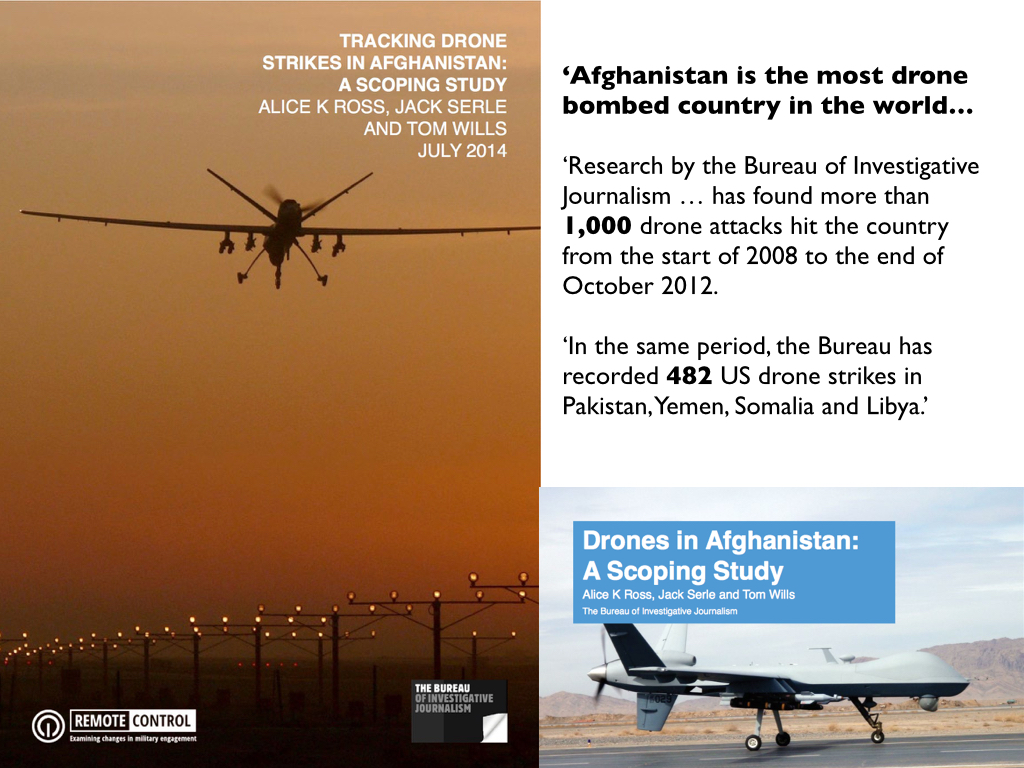
My larger project examines the evacuation of casualties, combatant and civilian, from four combat zones 1914-2014: the Western Front during the First World War, the deserts of North Africa during the Second World War, Vietnam, and Afghanistan.

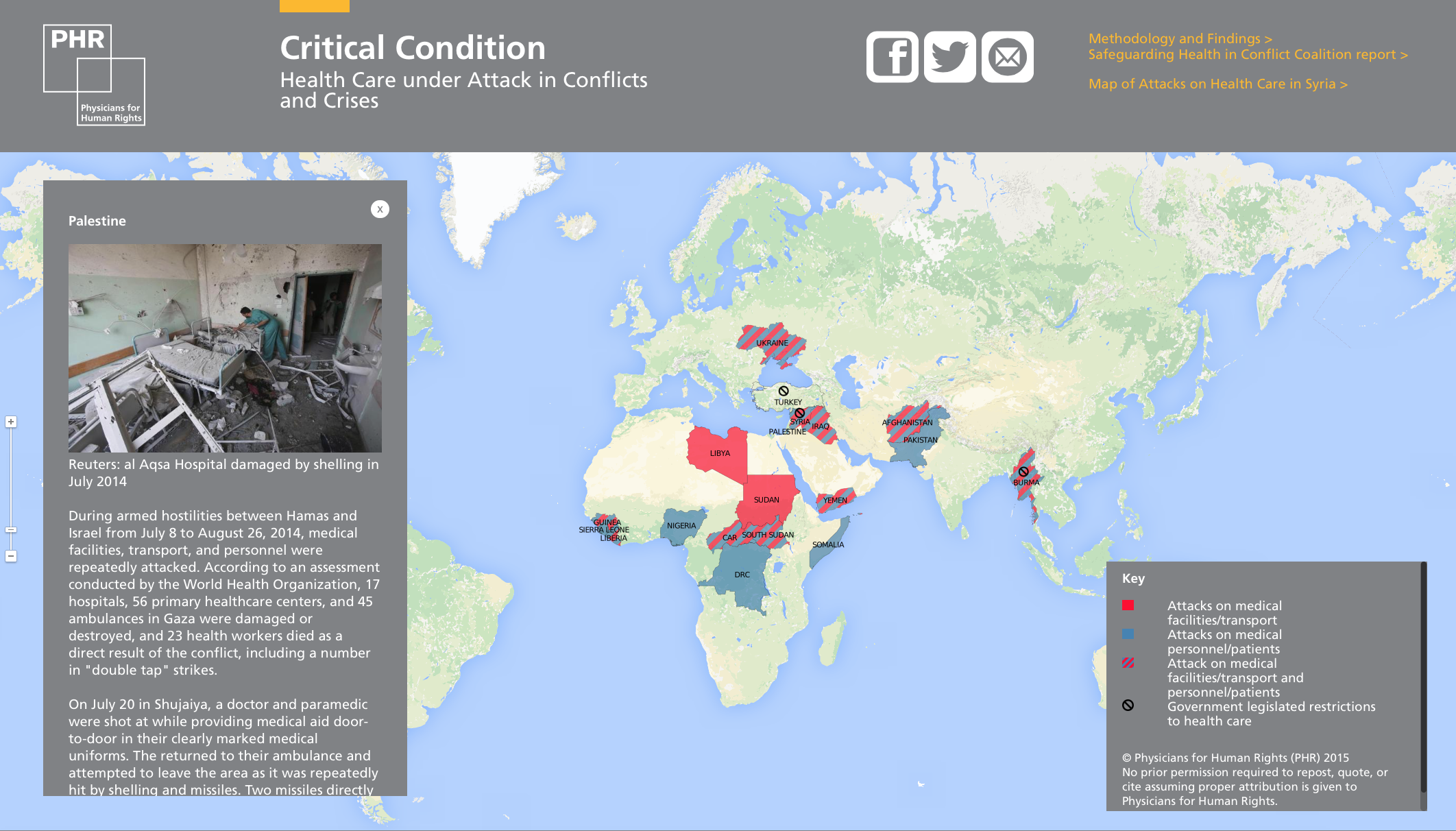
 As military and paramilitary attacks on hospitals and medical facilities have increased – in Afghanistan, Gaza, Syria, Yemen and elsewhere – even as the number of casualties has soared, Michael VanRooyen‘s new book The World’s Emergency Room (out next month from St Martin’s) promises to provide an urgent overview of what has become a routinised violation of medical neutrality:
As military and paramilitary attacks on hospitals and medical facilities have increased – in Afghanistan, Gaza, Syria, Yemen and elsewhere – even as the number of casualties has soared, Michael VanRooyen‘s new book The World’s Emergency Room (out next month from St Martin’s) promises to provide an urgent overview of what has become a routinised violation of medical neutrality: