I’ve noted on several occasions the multiple ways in which later modern war invokes medical metaphors to legitimise military violence (notably ‘surgical strikes’ against the ‘cancer’ of insurgency), and my preliminary work on medical-military machines has revealed all sorts of feedbacks between (in particular) trauma care by advanced militaries in war zones and trauma care by civilian agencies at home.

But these two paths have now intersected: in a paper on ‘Automated killing and mediated caring‘ Kathrin Friedrich and Moritz Queisner draw on studies of remote platforms and visual technologies – including my own – to discuss the automated killing of tumour cells using the CyberKnife system and what they call the the techno-medical ‘kill-chain’ that mediates between physician and patient. They write:
Gregory uses the term kill-chain to characterize the setting of military interventions by unmanned aerial systems as “a dispersed and distributed apparatus, a congerie of actors, objects, practices, discourses and affects, that entrains the people who are made part of it and constitutes them as particular kinds of subjects.” Image-guided interventions in medical contexts share similar structural features and are also characterized by tying together a heterogeneity of practices, actors, discourses and expertise in order to achieve a precisely defined goal but without obviously stating their inner relations and micro politics.

Their central question, appropriately re-phrased, can also be asked of today’s remote operations in theatres of war (and beyond):
The fact that medical robots increasingly determine medical therapy and often provide the only form of access to the operation area requires us to conceptualize them as care agents rather than to merely conceive of them as passive tools. But if the physician’s action is based on confidence in and cooperation with the robot, what kind of operative knowledge does this kind of agency require and how does it change the modalities of medical intervention?
They conclude:
… since surgical intervention has become a computer-mediated practice that inscribes the surgeon into a complex setting of medical care agents, it is no longer the patient’s body but the image of the body that is the central reference for the surgeon.
As the operator of robot-guided intervention the physician accordingly needs to address and cope with the specific agency of the machine. In addition the visual interfaces need to communicate and convert their technological complexity to humanly amendable surfaces.
I recommend reading these arguments and transpositions alongside Colleen Bell‘s ‘War and the allegory of military intervention: why metaphors matter’, International political sociology 6 (3) (2012) 325-28 and ‘Hybrid war and its metaphors’, Humanity 3 (2) (2012) and Lucy Suchman‘s ‘Situational awareness: deadly bioconvergence at the boundaries of bodies and machines’ (forthcoming at Mediatropes)…
There is yet another dimension to all this. The U.S. Army has been at the forefront of telemedicine for decades – for a recent report on ‘4G telemedicine’ see here – but since at least 2005 the Army has also been experimenting with ‘telesurgery’ or ‘remote surgery’ in which a UAV platform mediates between the surgeon and the site of patient treatment: a different version of remote operations. You can find early reports here, here and here (‘Doc at a distance’) and a more general account of ‘Extreme Telesurgery’ here. Still more generally, there’s a wide-ranging review of US Department of Defense research into Robotic Unmanned Systems for Combat Casualty Care here.
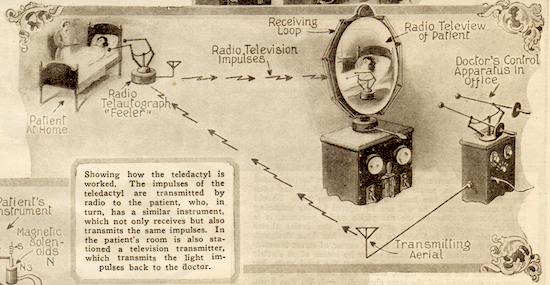
If this is all too futuristic – even ‘remote’ – to you, then check out the Teledactyl shown in the image below, which was originally published in 1925. Although there’s not a drone in sight, the seer was the amazing Hugo Gernsback, who also conjured up the radio-controlled television plane…