Happy New Year! With this, as with so much else, I’m late – but the greeting is none the less sincere, and I’m grateful for your continued interest and engagement with my work.
I’ve resolved to return to my usual pace of blogging in 2019; it slowed over the last several months, not least because I’ve been deep in the digital archives (apart from my merciless incarceration in Marking Hell and my release for Christmas).
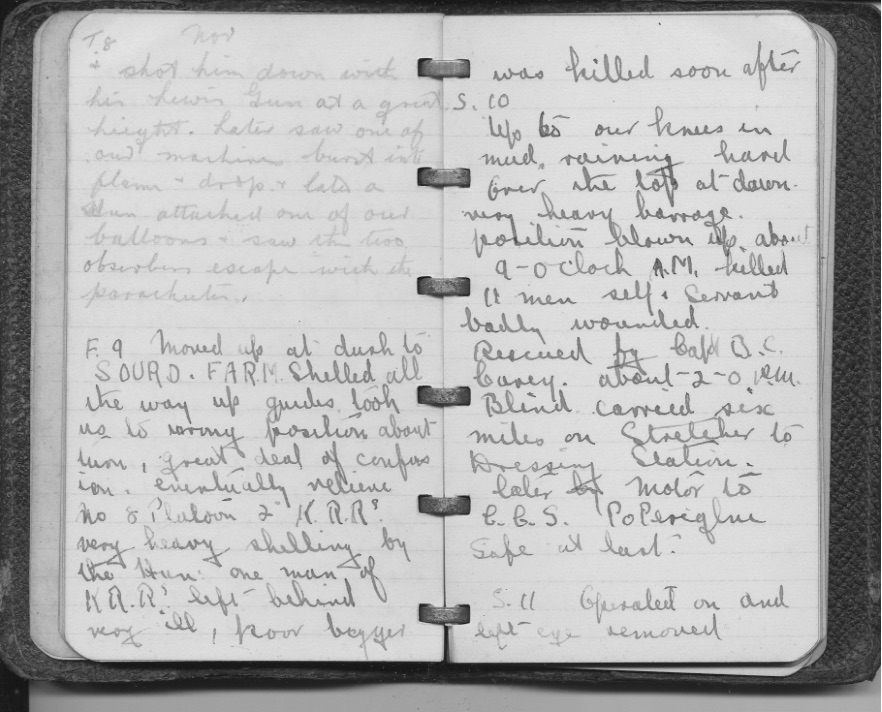
My plan is to finish two major essays in the next couple of months, one on “Woundscapes of the Western Front” and the other the long-form version of my Antipode Lecture on “Trauma Geographies” (see also here). Both have involved close readings of multiple personal accounts of the journeys made (or not made) by the wounded, and the first essay informs the second, as you can see here.
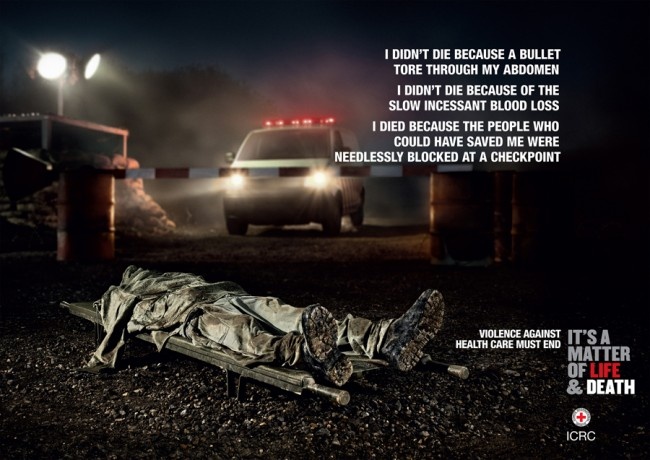
I also want to bring together my research on attacks on hospitals, casualty clearing stations and aid posts during the First World War in a third essay – I’ve been talking with the ICRC about this one. Paige Patchin managed to track down a series of files on the Etaples bombings in the National Archives for me, including an astonishing map plotting the paths of the enemy aircraft and the locations of the bombs: I’ll share that once I’ve managed to stitch together the multiple sheets. But I’ve widened the analysis beyond the attacks on base hospitals on the coast, to include other attacks – notably the bombing of the hospital at Vadelaincourt near Verdun – and a more general discussion of the protections afforded by the Red Cross flag and the Hague Conventions.

This will in turn thread its way into a fourth essay providing a more comprehensive view on violations of what I’ve called ‘the exception to the exception’: the disregard for the provisions of International Humanitarian Law evident in the attacks on hospitals and clinics in Afghanistan, Gaza, Syria and elsewhere, in short “The Death of the Clinic“.

That project interlocks with my developing critique of Giorgio Agamben‘s treatment of the “space of exception”. In brief:
- I think it’s a mistake to treat the space of the camp as closed (there is a profoundly important dispersal to the space of exception, evident in the case of Auschwitz that forms the heart of Agamben’s discussions – I’m thinking of the insidious restrictions on the movement of Jews in occupied Europe, the round-ups in Paris and other cities (see my lecture on Occupied Paris under the TEACHING tab), and the wretched train journeys across Europe to Poland – and this matters because if we don’t recognise the signs of exception at the peripheries they will inexorably be condensed inside the enclosure of the camp).
- It’s also unduly limiting to restrict the space of exception to the camp, because the war zone is also one in which people are knowingly and deliberately exposed to death through the removal of legal protocols that would otherwise have offered them protection (and here too what Frédéric Mégret calls ‘the deconstruction of the battlefield‘ emphasises the complex topology of the exception). I’ve written about this in relation to the Federally Administered Tribal Areas of Pakistan (see “Dirty Dancing” under the DOWNLOADS tab) and the conduct of siege warfare in Syria (multiple posts, listed under the GUIDE tab), but it’s a general argument that I need to develop further).
- In neither case – camp or war zone – is there an absence of law; on the contrary, these spaces typically entail complex legal geographies, at once national and – never discussed by Agamben – international (though part of my argument addresses the highly selective enforcement of international humanitarian law and the comprehensive contemporary assault on its provisions by Russia and Syria and by the United States, Israel and the UK, amongst others).
- In both cases, too, the space of exception is profoundly racialised (I’ve written about that in relation to the bombing of Japan in World War II and the contemporary degradations inflicted on prisoners at Abu Ghraib and Guantanamo – you can find the relevant essays under the DOWNLOADS tab – but I’ve found Alexander Weheliye‘s Habeas Viscus: Racializing Assemblages, Biopolitics, and Black Feminist Theories of the Human immensely helpful in deepening and generalising the argument).
I’ll be developing these arguments in my KISS Lecture at Canterbury in March, which ought to form the basis for a fifth essay (and it’s also high time I revisited what I said in “The everywhere war”!).
More on those projects soon, all of which will feed in to two new books (once I’ve decided on a publisher – and a publisher has decided on me), but in the interim I’ll be sharing some of the drafts and jottings I’ve prepared en route to the finished essays.
So lots to keep my busy, and I hope you’ll continue to watch this space – and, as always, I welcome comments and suggestions.