In what now seems another life, I wrote about US torture during the early years of the “war on terror”, in ‘The Black Flag’ (which was specifically about Guantanamo, and which opened with three ‘suicides’ that we now have good reason to believe were anything but: see here and here) and ‘Vanishing Points’ (which extended the argument to Abu Ghraib and the archipelago of black sites like the ‘Salt Pit’ [shown below] within the global war prison). Both are available in their original forms under the DOWNLOADS tab, and form part of the material I’ve been working with for a new essay to be included in The everywhere war.
Now I’m digesting the Executive Summary that has been released by the Senate Select Committee on Intelligence on the CIA’s Detention and Interrogation Program, but you can download the original (redacted) summary here, ‘Other Views’ here, and the Minority View from the Republicans – and please God it remains a minority view – here.
The New York Times‘ coverage is here, the Washington Post‘s here, and the Guardian‘s here.
In the meantime, some of the best work on the dispersed geography of this vast apparatus was carried out by Trevor Paglen (see my updated discussion here).
Readers of his Blank spaces on the map will know of Trevor’s own attempt to see the ‘Salt Pit’ for himself, on the ground rather than from the air, and the images that result from this dimension of his work make clear – in plain sight, so to speak – their constitutive difficulties: see, for example, Jonah Weiner‘s essay on his work, ‘Prying eyes’, that appeared in the New Yorkerhere.
But here is part of what Trevor had to say about the mappings like the one above involved in his Torture Taxi and Terminal Air projects in An Atlas of Radical Cartography:
I’ve actually tried to stay away from cartography and “mapping” as much as possible in my work. The “God’s eye” view implicit in much cartography is usually not helpful in terms of describing everyday life, nor in describing the qualities of the relationships that cartography depicts. Because of what cartography cannot represent… it becomes pretty clear why it (and the forms of power that the cartographic viewpoint suggests) have traditionally been such powerful instruments of both colonialism and the contemporary geopolitical ordering of the world (which of course very much comes out of colonialism)…
I tend to be far more attracted to “on the ground” viewpoints and to embrace their fragmentedness and incompleteness. This project, as well as the “Terminal Air” project with the Institute for Applied Autonomy, are of course notable exceptions. With both of these projects that use the cartographic viewpoint, I was interested in taking what might seem like a familiar image and trying to and make it strange – trying to capture the feeling I had when I first started following CIA flights: it was the constant domestic flights to places like Tulsa, Las Vegas, Fresno, Fort Lauderdale and such that made a big impression on me. In working with John Emerson and the IAA, I insisted that we try to show a continuum between the domestic landscape and the landscape “somewhere else.” Neither of these projects are in my view not particularly useful as didactic tools but are instead useful in helping to see the point that we talked about above: that the “darkest” spaces of the war on terror blur into the everyday landscapes here “at home” and are in many way mutually constitutive. In this sense, they’re … images rather than analytic tools.
As I’ve noted before, this is part of the ‘capture’ side of the US kill-capture apparatus that uses drones (and often Special Forces) for the ‘kill’. I say ‘US’, but it’s clear – not least from the map above – that a network of other states that radiates far beyond the other ‘Five Eyes‘ which have been so deeply involved in providing geospatial intelligence for drone strikes (and more) has been complicit in the production and concealment of this global archipelago of torture.
But there’s an irony in all this: even as the Obama administration ramped up drone strikes – and after a lull they have been resumed with a vengeance in Pakistan’s Federally Administered Tribal Areas – it was also condemning torture and, last month, committed the United States to acknowledging the extraterritorial reach of the Convention Against Torture (see Sarah Cleveland at Just Security here and Ryan Goodman and Eric Messengerhere). The refusal of the Bush administration to do so was a central part of the argument about legal geographies that I developed in both ‘The Black Flag’ and ‘Vanishing Points’.
So now we have an administration that recognises extra-territoriality to proscribe torture – and insists on it (or its own version of extra-territoriality) to authorise targeted killing.
This is worryingly authoritarian, bad for public health, and strategically counterproductive. Despite its impressive logistics, the army makes only a marginal contribution to international disaster relief — and often makes things worse. Nor do soldiers “fight” pathogens — and the language of warfare risks turning infected people and their caretakers into objects of fear and stigma.
Even brave and compassionate civilian fieldworkers are not immune from the military metaphors. Here, for example, is Sarah Crowe of UNICEF describing her work on the ‘frontline’ in Liberia’s ‘biological war’:
‘Ebola has turned survivors into human booby traps, unexploded ordnance – touch and you die. Ebola psychosis is paralysing…
‘In the car with colleagues, they talk almost nostalgically about the long civil war here – a time when the enemy was seen, the rockets were heard, the bullets could be dodged.’
If you want refuge from the paranoid hallucinations about the non-metaphorical weaponisation of Ebola by either the United States or ISIS read (respectively) Jim Whitehere and Scott Stewarthere.
Back to Alex, who provides a crucial and extremely helpful gloss on the recent history of US research on the intersections between epidemic disease and national security, which shows:
Modern epidemics do not cause security crises… Newly evolved pathogens are a constant threat, but a rerun of the near-total devastation of the native American populations by diseases entirely new to them is far-fetched for the simple reason that there are no longer any large populations wholly isolated from, and therefore at risk of, major infections. The greater dangers come from panicked or coercive responses to disease.
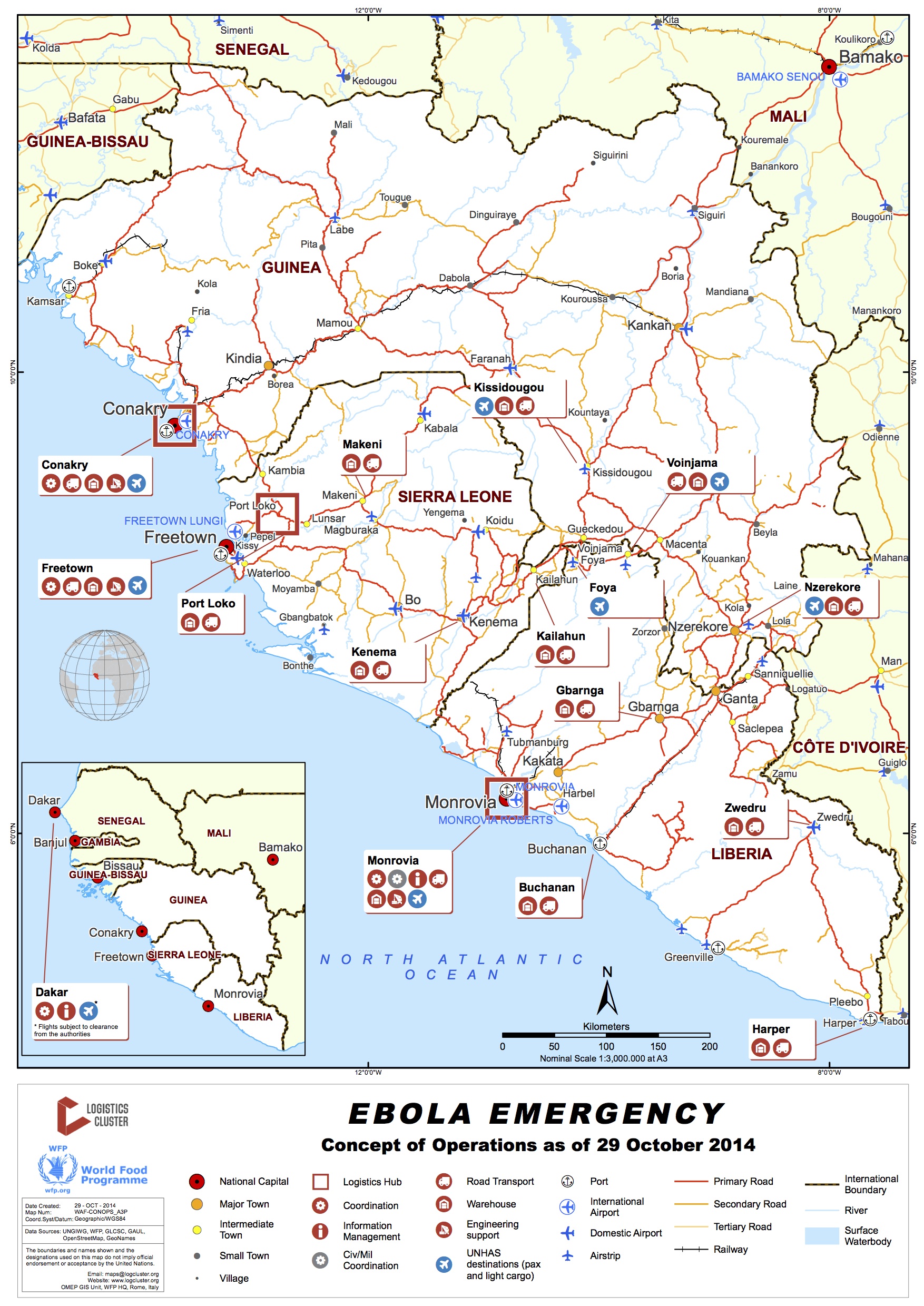
And for all the attempts to securitise Ebola, there has been remarkably little attention paid to its implications for food security (an altogether different problematic). Here the work of the Assessment Capacities Project (ACAPS), an initiative of Action Contre la Faim, the Norwegian Refugee Council and Save the Children International, is exemplary – see their detailed Briefing Note, Ebola in West Africa: potential impact on food security (10 November), from which I’ve taken the map below (there are others in the Note).
Alex points out another problem with the militarization of public health: ‘the legacy of colonialism and coercive medicine.’
Best practices in global health include efforts to be sensitive to national histories and cultures and to overcome the suspicions induced by outside health programs. Medicine in khaki is not only inefficient, it is bad practice.
British, French, and American armies have a history of imposing control in the name of hygiene, cordoning off a city or as-yet-insufficiently governed parts of the global borderlands…. In much of Africa, public health has struggled to free itself from the way it was implicated in coercive colonial control measures.
It is precisely this insight that eludes Tom Koch in his discussion of the history of mapping and containing epidemic disease in general and Ebola in particular. ‘It’s not “like” wartime,’ he proclaims: ‘It is war.’
To combat the expanding bacterium or an advancing, viral incursion has always required military style thinking. To survive, a microbe requires potential hosts who can be effected just as invading armies require supplies if they are to advance. To tame a microbial incursion requires containment procedures that will deny it new hosts, new supplies.
He is right to point to the strategic importance of mapping – on the National Geospatial Intelligence Agency’s public involvement, incidentally, see here – but maps (like metaphors) do more than describe, and depending on the web of practices and powers in which they are activated the connections between mapping and containment are in many cases performative. I’m surely not the only one to be reminded of Michel Foucault‘s illuminating discussion of the plague-stricken town: see also Stuart Elden‘s commentary on ‘Plague, Panopticon, Police’ here, which reinforces the suggestions I made about military/policing and quarantine in my original post. But this involves more then AFRICOM, and Donald McNeil‘s report on the decision to use local militaries to impose a cordon sanitaire in areas of Liberia and Sierre Leone (below) is also instructive – as he says, ‘a tactic unseen in a century’ and with ‘the potential to become brutal and inhumane’.
It may also backfire. Alex again (my emphases):
One of the great, under-recognized successes of the response to HIV and AIDS in Africa was that the spread of an incurable sexually transmitted infection did not lead to repressive measures or massive stigmatization. On the contrary, the United Nations and donors insisted that public health be linked to human rights, and civil society organizations and people living with HIV and AIDS be represented in the governance of UNAIDS and the Global Fund.
That is the polar opposite of the war-like approach to Ebola. The Sierra Leonean journalist Oswald Hanciles drew out the implications of Koroma’s “war” on Ebola, comparing it favorably with the weak government defenses against the rebel attacks fifteen years ago: “This strategy of energizing and mobilizing youth to ‘comb’ their neighborhoods to ferret out ‘Ebola suspects’ could be the most potent in this Ebola War. We are optimistic that the President would use the security forces to back up the youths who the President said should be ‘hard.’” That would be a frightening prospect. Vigilante mobs dragging people from their homes or sealing off neighborhoods would destroy the public trust and community involvement at the heart of good public health practice.
It’s not only vigilante mobs; the image below shows a Liberian soldier beating a local resident while enforcing a quarantine in Monrovia’s West Point slum:
And yet several loud voices doubt that local militaries, even acting in concert with AFRICOM, can provide a sufficiently powerful vector, and they want the militarised response to be stepped up. Earlier this month Britain’s former Chief of the Defence Staff joined calls for NATO to take command:
General Sir David Richards said that he was “strongly supportive” of a proposal for Nato to take command of the international response to West Africa’s Ebola outbreak, adding that the crisis demanded “a grand strategic response…
“What a crisis like this requires more than anything else is efficient organisation and leadership. It is quite clear that currently these vital ingredients are missing… The military’s core skills are to analyse a problem, devise a plan … and then to execute that plan under pressure.”
It may be that the ‘organisation and leadership’ they have in mind is a matter of logistics. The United Nations has a Global Logistics Cluster, whose ‘concept of operations’ is mapped below (see also its Regional Situation Report for 3-10 November here) , and Richards and his co-signatories make it plain that, in their view, the UN is ‘most unlikely to be up to the job’ – though they never clarify exactly what that ‘job’ might be and what they expect NATO to do. In any case, readers of Deb Cowen may well wonder about another dimension of what she calls ‘the deadly life of logistics’…
So I leave the last word to Alex:
The comparative advantage of the military lies in a few niche activities, such as airport infrastructure, transport helicopters, and — uniquely for this case — medical facilities to treat health workers when they themselves fall sick. All other activities are done far better by civilians.
We’ve been here before – ‘wars’ on this and ‘wars’ on that. It’s strange how reluctant states are to admit that their use of military violence (especially when it doesn’t involve ‘boots on the ground‘) isn’t really war at all – ‘overseas contingency operations’ is what the Pentagon once preferred, but I’ve lost count of how many linguistic somersaults they’ve performed since then to camouflage their campaigns – and yet how eager they are to declare everything else a war.
These tricks are double-edged. While advanced militaries and their paymasters go to extraordinary linguistic lengths to mask the effects of their work, medical scientists have been busily appropriating the metaphorical terrain from which modern armies are in embarrassed retreat.
Yet all metaphors take us somewhere before they break down, and the ‘war on Ebola’ takes us more or less directly to the militarisation of the global response. In an otherwise critical commentary, Karen Greenberg draws parallels between the ‘the war on terror’ and the ‘war on Ebola’:
‘The differences between the two “wars” may seem too obvious to belabor, since Ebola is a disease with a medical etiology and scientific remedies, while ISIS is a sentient enemy. Nevertheless, Ebola does seem to mimic some of the characteristics experts long ago assigned to al-Qaeda and its various wannabe and successor outfits. It lurks in the shadows until it strikes. It threatens the safety of civilians across the United States. Its root causes lie in the poverty and squalor of distant countries. Its spread must be stopped at its region of origin — in this case, Guinea, Liberia, and Sierra Leone in West Africa — just as both the Bush and Obama administrations were convinced that the fight against al-Qaeda had to be taken militarily to the backlands of the planet from Pakistan’s tribal borderlands to Yemen’s rural areas.’
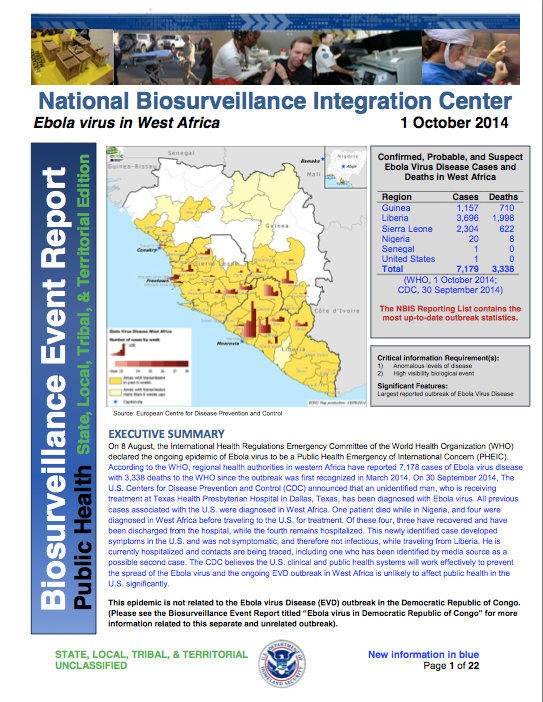
There are other parallels too, not least the endless re-descriptions of terrorism and even insurgency as life-threatening diseases, ‘cancers’ on the body politic. And, as Josh Holmesshows, there is also an entirely parallel (geo)politics of fear in both cases (see also Rebecca Gordon on the racialization of ‘the fear machine’ here). Given the threat supposedly posed by ‘the enemy within’, it’s not surprising that US Northern Command has already set up a 30-person ‘military rapid response team‘ for domestic Ebola cases, and that the Department of Homeland Security has been issuing Biosurveillance Event Reports on the Ebola outbreak in West Africa from the National Biosurveillance Integration Center.
But as I’ve said, Karen’s is a critical commentary and so, before the military metaphors carry us away, her conclusion bears repeating:
The United States is about to be tested by a disease in ways that could dovetail remarkably well with the war on terror. In this context, think of Ebola as the universe’s unfair challenge to everything that war bred in our governmental system. As it happens, those things that the U.S. did, often ineffectively and counterproductively, to thwart its enemies, potential enemies, and even its own citizenry will not be an antidote to this “enemy” either. It, too, may be transnational, originate in fragile states, and affect those who come in contact with it, but it cannot be stopped by the methods of the national security state.
To make sense of all this, I think we need to stand back and start with four general observations:
(1) Modern military medicine has long involved more than evacuating and treating the wounded from the field of battle. It has always had a substantial public health component. Until the early twentieth century, ‘infectious diseases unrelated to trauma were responsible for a much greater proportion of the deaths during war than battle-related injuries‘. As militaries started to pay much closer attention to hygiene and disease prevention, Matthew Smallman-Raynorand Andrew Cliff estimate that the ratio of ‘battle deaths’ to deaths from disease amongst the military population fell from 1:0.4 in the First World War to 1:0.1 in the Second World War; then it rose to 1:0.13 in the Vietnam War but in the first US-led Gulf War (1991) it fell to 1:0.01.
(2) Modern militaries are no strangers to biowarfare either. Both sides in the First World War experimented with chemical weapons, and although the US Army’s explicitly offensive Biological Warfare Weapons Laboratories closed in 1969 the commitment to ‘bio-defense’ and bio-security has ensured a continuing military investment in the weaponisation of infectious diseases (see right). I don’t subscribe to the view that the Ebola epidemic in West Africa is the result of a rogue US biowarfare program – see for example the claims made by ‘Robert Wenzel’here: and if you want to know why his name is in scare-quotes, appropriately enough, read Chris Becker‘s takedown here – nor to the fear that what Scientific Americancalls ‘weaponised Ebola’ is poised to become a ‘bio-terror threat’. But I do think it worth noting the work of the US Army Medical Research Institute of Infectious Diseases which has had field teams on the ground in West Africa since 2006, and the importance placed on surveillance and monitoring.
(3) I also think it’s necessary to think through the biopolitics of public health in relation to military and paramilitary violence. This takes multiple forms. It’s become dismally apparent that in many conflict zones hospitals, doctors and other health-care workers have become targets: in Gaza, to be sure, but in Syria and elsewhere too. The treatment of disease has also become a tactical vector: think of the CIA’s use of polio vaccination campaigns as a cover for its intelligence operations and – the conjunction is imperative – the Taliban’s manipulation of polio vaccinations in Pakistan’s Federally Administered Tribal Areas. Think, too, of the way in which the Assad regime has inflicted a resurgent, even counterinsurgent geography of polio on the Syrian people. As Annie Sparrowshows (see also here):
‘This man-made outbreak is a consequence of the way that Syrian President Bashar al-Assad has chosen to fight the war—a war crime of truly epidemic proportions. Even before the uprising, in areas considered politically unsympathetic like Deir Ezzor, the government stopped maintaining sanitation and safe-water services, and began withholding routine immunizations for preventable childhood diseases. Once the war began, the government started ruthless attacks on civilians in opposition-held areas, forcing millions to seek refuge in filthy, crowded, and cold conditions. Compounding the problem are Assad’s ongoing attacks on doctors and the health care system, his besieging of cities, his obstruction of humanitarian aid, and his channeling of vaccines and other relief to pro-regime territory.
‘… nearly all the cases of polio have occurred in areas of northern Syria under rebel control, where the government is seemingly doing everything in its power to prevent vaccination. The Syrian government has appealed to the UN for hundreds of medicines for areas of the country it controls, while largely ignoring the far more dire needs of opposition-held areas. Many children, especially newborns, still do not have access to polio immunization. Daily government airstrikes target the very health facilities that should be the foundation of vaccination efforts, as well as the children who should be protected from polio, measles, and other preventable childhood diseases. As Dr. Ammar, a doctor from Aleppo, said to me bitterly after an April 30 airstrike killed twenty-two schoolgirls, “The government’s polio control strategy for children is to kill them before they can get polio.”’
In her original essay, Sara shows how powerful states in the global North joined forces with the World Health Organisation to construct infectious disease as an existential security threat that demanded new rules and protocols for its effective containment. Crucially:
‘The outcome of this has been the development of international health cooperation mechanisms that place western fears of an outbreak reaching them above the prevention of such outbreaks in the first place. In turn, the desire of the WHO to assert its authority in the project of disease surveillance and containment has led it to develop global health mechanisms that primarily prioritizes the protection of western states from disease contagion.’
This has a genealogy as well as a geography (or what Alan Ingram once called a ‘geopolitics of disease’). Peter Dörrienotes that on 18 September 2014 the U.N. Security Council declared the current Ebola outbreak in West Africa ‘a threat to international peace and security’, and that this was ‘the first time the U.N. had taken this step in a public health crisis‘ (in fact the Council had previously expressed similar concerns about the impact of HIV/AIDS on ‘stability and security’). Under Chapter VII of the UN Charter this declaration has significant legal implications, as Jens David Ohlin notes here, but what most concerns Peter is how long it took for the Security Council to stir itself. It issued its statement 180 days after the WHO confirmed the outbreak, and over a month after the WHO had declared Ebola a ‘Public Health Emergency of International Concern’, and in his eyes the international system ‘ignored the problem until it was too big for any solution other than full-scale military intervention.’ But I’ve already suggested, it’s wrong to treat the militarisation of epidemic disease as somehow new. Of direct relevance to the present ‘war on Ebola’ is this passage from Sara’s essay:
The United States has been a keen participant in disease surveillance and response since the mid-1990s. The United States Department of Defense (US DoD) has had overseas infectious disease research laboratories located in over 20 countries for nearly ten years. The Global Emerging Infectious Surveillance and Response System (DoD-GEIS) mobile laboratories were set up for the purpose of ‘responding to outbreaks of epidemic, endemic and emergent diseases’, and their location in the DoD, as opposed to the United States Agency for International Development (USAID) or Centre for Disease Control (CDC) demonstrates how seriously the United States views the response to infectious disease as a key national security strategy.
So, four observations about the military-medical-security nexus that provide a context for the ‘war on Ebola’. There are two other issues that should also be on the table before proceeding.
The first involves the imaginative geographies circulating in the global North that (mis)inform public response to the epidemic. Many of them can be traced back to colonial descriptions of the coast of nineteenth-century West Africa (and Sierra Leone in particular) as ‘the white man’s grave’, a form of what in a different context Dan Clayton calls a ‘militant tropically’. The contemporary reactivation of these tropes is clearly a serious concern because it corrodes an effective political response. As geographer Kerrie Thornhill writes,
African and diaspora scholars, already accustomed to the ‘thousand tiny paper cuts’ of casual racism, demonstrate how these (metaphorical) cuts escalate into real fatalities. Writers such as Nanjala Nyabola and Lola Okolosie point out the abundance of racist tropes depicting West African societies as inherently unclean, chaotic, uncooperative, ungrateful, and childlike. This racism reinforces a global culture of disregard for black African lives, and the perception that they are a source of social and biological contamination.
You can find much more on this in Cultural Anthropology‘s brilliant Ebola in Perspective series.
The second is the precarious condition of health care systems in West Africa (Ebola in Perspective is good on this too). Brice de la Vigne, the operations director of MSF, reminds us that ‘both Sierra Leone and Liberia were at war ten years ago and all the infrastructure was destroyed. It’s the worst place on earth to have these epidemics.’ Other critics suggest that these uncivil wars were not the only culprits. In their view, it was the neoliberal economic model forced on West Africa by the global North that was primarily responsible for gutting public health systems:
While years of war played a role in weakening public systems, it is the “war against people, driven by international financial institutions” that is largely responsible for decimating the public health care system, eroding wages and conditions for health care workers, and fueling the crisis sweeping West Africa today, says [Emira] Woods. “Over the past six months to a year there have been rolling health care worker strikes in country after country—Nigeria, Sierra Leone, and Liberia,” said Woods. “Nurses and doctors are risking and losing their lives but don’t have protective gear needed to serve patients and save their own lives. They are on the front lines and have not had their voices heard.”
So – back to the front lines. Despite the geopolitical-military-security back story, it was Médecins Sans Frontières that made the first public call (on 2 September) for military assistance in combatting Ebola.
‘States with biological-disaster response capacity, including civilian and military medical capability, must immediately dispatch assets and personnel to West Africa…
‘Many countries possess biological threat response mechanisms. They can deploy trained civilian or military medical teams in a matter of days, in an organised fashion, and with a chain of command to assure high standards of safety and efficiency to support the affected countries…
‘In the immediate term, field hospitals with isolation wards must be scaled up, trained personnel must be dispatched, mobile laboratories must be deployed to improve diagnostics, air bridges must be established to move personnel and material to and within West Africa, and a regional network of field hospitals must be established to treat medical personnel with suspected or actual infections.’
Ten days later Peter Piot, the Director of the London School of Tropical Medicine and Hygiene and the microbiologist who helped identify the Ebola virus in 1976, also called for a ‘quasi-military intervention’. Although he spoke about a ‘state of emergency’, he too wanted to reverse the response prefigured by Giorgio Agamben in such situations and contract the spaces of exception that were multiplying across West Africa. He had in mind ‘beds, ambulances and trucks as well as an army of clinicians, doctors and nurses.’
What materialised was rather different.
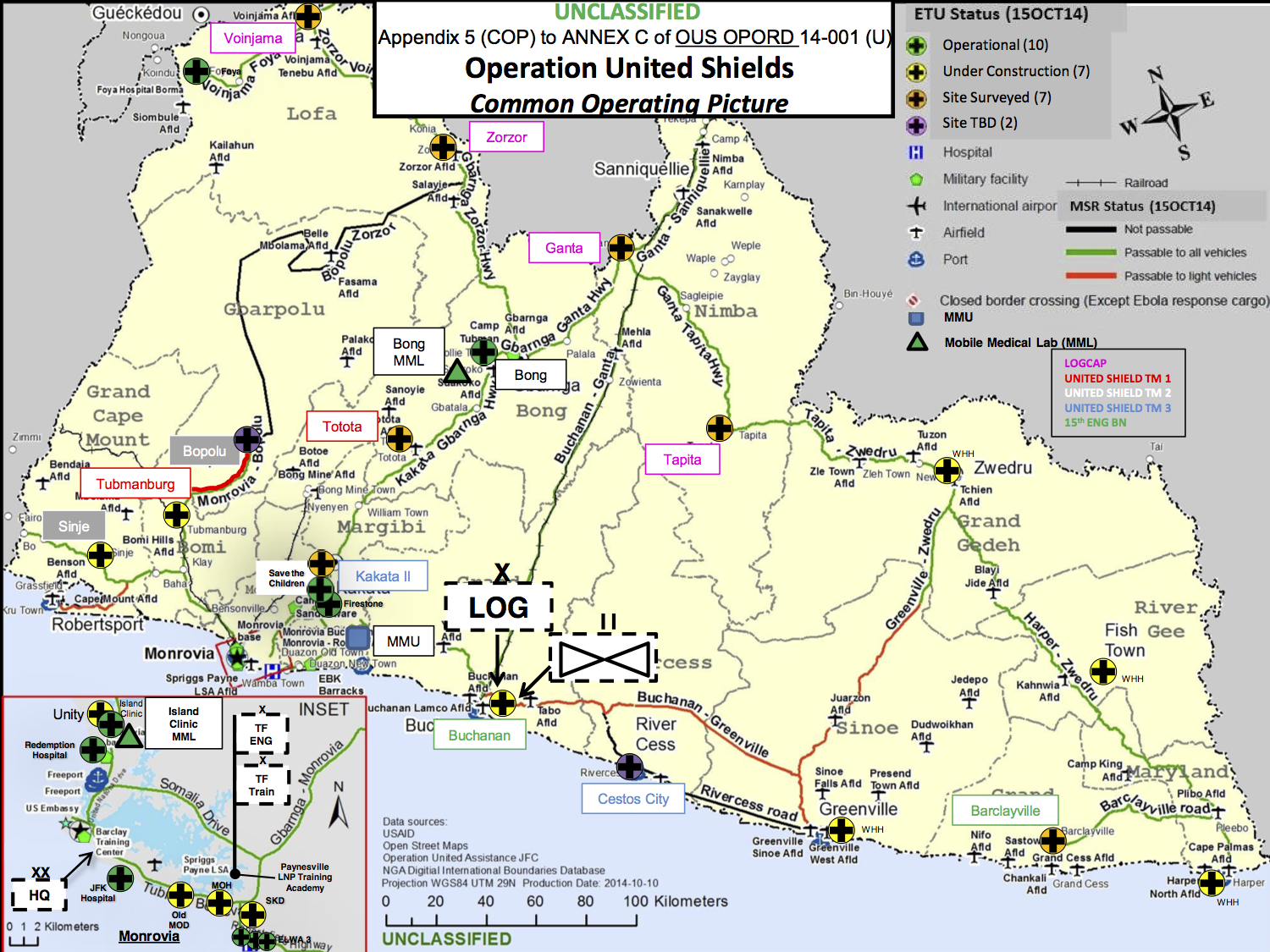
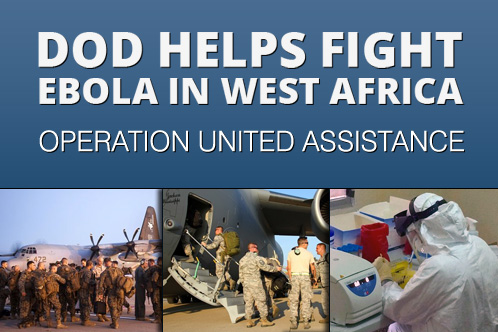
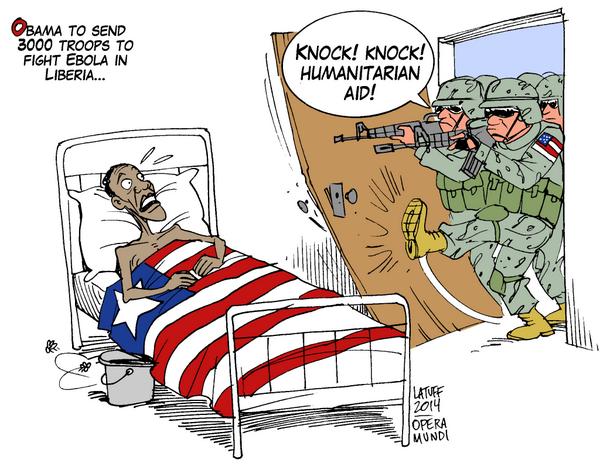
On 16 September President Obama flew to the Centers for Disease Control and Prevention in Atlanta to announceOperation United Assistance. He committed 3-4,000 US troops and $750 million in defence funding to the mission, which is being orchestrated by US Africa Command (AFRICOM) through US Army Africa in concert with USAID. The focus of the US military-medical mission is Liberia. There are close historical connections between the US and Liberia, which originally offered to host AFRICOM’s headquarters in the capital Monrovia; now a Joint Force Command has been set up there. You can find the 75-page AFRICOM operational order here, dated 15 October 2014, from which I’ve taken the ‘common operating picture’ below. The title puzzles me – the only ‘Operation United Shield’ (singular) I’ve been able to find was a multinational operation to evacuate peacekeeping forces from Somalia in 1995. Appendix B is particularly worth reading, incidentally, because it identifies ‘the enemy’: ‘Ebola Virus Disease is the enemy, aided by poor preventive medicine practices in areas where EVD cases are prevalent and difficulties in identifying and treating EVD patients.’
The US deployment is complemented by the deployment of UK forces to Sierra Leone (Operation Gritrock)and French forces to Guinea. In both cases there are also close, colonial connections, and the British-led International Military Advisory Training Team Sierra Leone has been on the ground since 2000 (since last year this has been re-tasked as the International Security Advisory Team Sierra Leone).
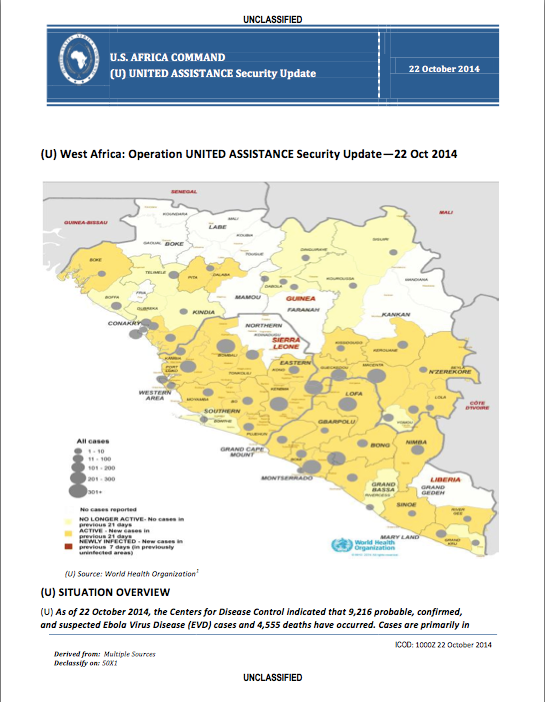
(The map above is borrowed from the BBC; in addition, the Guardian has an interactive map tracing the historical geography of Ebola from the first known case in the Democratic Republic of Congo in 1976 to the present epidemic in West Africa here).
These forces differ in more than geographical deployment; their capabilities differ significantly too. The UK is sending 750 troops, including contingents from the Royal Army Medical Corps (notably 22 Field Hospital), who will construct treatment centres (the aim is to add 700 beds to triple Sierra Leone’s existing capacity) and treat doctors and other health-care workers who contract the disease; they are supported by the Royal Navy’s ‘Primary Casualty Receiving Ship’ RFA Argus (which will provide a further 100 beds), and by another 780 volunteer health care staff.
The US has mobilised troops from the 101st Airborne, whose primary mission is to set up 17 Ebola Treatment Units (each with 100 beds); meanwhile the US Air Force’s 633rd Medical Group is establishing a 25-bed Expeditionary Medical Support System field hospital for doctors and other health care workers who contract the disease (below). The US Army has also fielded three mobile laboratories to test samples for the virus, reducing the time to diagnosis from days to hours. According to Pardis Sabeti, who leads viral-genome research at the Broad Institute of M.I.T. and Harvard, ‘the faster you can get a diagnosis of Ebola, the faster you can stop it.’
‘Our enemy is a disease’, declared Lt Col Brian De Santis, echoing AFRICOM’s operational order – but it was quickly made clear that the vast majority of troops will not come into contact with the enemy or any of its victims at all. This is just as well; most of the soldiers have minimal medical training – just four hours from the US Army Medical Research Institute of Infectious Disease – and the Pentagon’s Press Secretary Rear Admiral John Kirbyexplained that there is ‘no intention right now that [troops] will interact with patients or be in areas where they would necessarily come into contact with patients’:
‘They’re not doctors. They’re not nurses. They’re not trained for that and not equipped for that. That’s not part of the mission. They will be kept in locations where they can do their jobs without coming into contact with patients.’
‘It’s like the city that spends all its money to raise up a formidable police force only to discover that what it really needs is a bigger sewage treatment plant. Of course, you can always put cops to work burning human excrement but there are better — that is, more effective and cheaper — ways to solve the problem.’
In effect, this is another case of the military preferring remote operations. Here is a telling passage from Sophie Arie’s interview with MSF’s president Joanne Liu:
‘“Countries are approaching this with the mindset of going to war,” she says. “Zero risk. Zero casualties.” Liu describes the current military efforts as the equivalent, in public health terms, of airstrikes without boots on the ground. Pledges of equipment and logistical support are helpful—“The military are the only body that can be deployed in the numbers needed now and that can organise things fast.” But there is still a massive shortage of qualified and trained medical staff on the ground. “You need to send people not stuff and get hands on, not try to do this remotely,” Liu says…’
The primary areas for military operations in the ‘war on Ebola’ to date are surveillance, logistics and containment. I’ll consider each in turn.
Last week Public Intelligencereleased a series of weekly Security Updates and daily Intelligence Summaries produced by AFRICOM to support Operation United Assistance. These rely largely on WHO reporting to track the spread of the disease.
This is to work at a highly aggregate level. Most public health experts suggest that the key to stopping the spread of the disease is contact tracing – which, in its essentials, is the same methodology used by the military and the intelligence services to track individuals through terrorist and insurgent networks – and has been used successfully in both the United States and in Nigeria (which was declared free of Ebola on 20 October). Ezra Kleindescribes it as ‘almost ludicrously simple’ and ‘as low-tech as medicine gets’, and so it is in principle.
But its application in much of West Africa is immensely difficult: the UN estimates that only 16 out of 44 zones have adequate procedures and personnel in place. And since many local people are understandably fearful of the consequences of their answers, it is unlikely that military involvement would improve the situation. Here is Elizabeth Cohen and John Bonifield:
‘People are often uncooperative with the tracers, sometimes even throwing stones at health care workers. They fear that they or their loved ones will be put in the hospital; they’ve seen firsthand that people who go there often don’t return.
“The community perceives this as a death sentence,” [Donald Thea, an infectious disease epidemiologist] said. “Relinquishing your loved one is tantamount to death.”
And health care workers have very little to offer people as an incentive to cooperate. “With smallpox, we could offer people a vaccine, a carrot in essence to induce them to be cooperative. With Ebola, we have nothing,” Thea said.’
Logistics is the area where the military comes into its own. MSF had emphasised that its priorities included ‘the mass expansion of isolation centers, air bridges to move personnel and equipment to and within the most affected countries, mobile laboratories for testing and diagnosis, and building a regional network of field hospitals to treat suspected or infected medical personnel.’ Much of the military effort is currently concentrated in these areas, but the other side to mobilising medical personnel, equipment and testing and treatment facilities is, in effect, immobilising the population.
Containment runs the gamut from quarantine through curfews and lockdowns to border closures. Most observers believe that border closures would be counter-productive: if you want to know why, see Debora MacKenzie‘s short essay here. The other, seemingly lesser measures also have their dangers. In its original call for assistance, MSF insisted that ‘any military assets and personnel deployed to the region should not be used for quarantine, containment, or crowd control measures’, and it emphasised that ‘forced quarantines have only bred fear and unrest, rather than stem the virus.’
But others have other ideas. Major Matt Cavanaugh, from the US Army War College, has made an unofficial, back-of-the-envelope calculation of what a successful ‘containment strategy’ for Ebola would require. He is adamant that only ‘boots on the ground’ could do the job, though the nature of that ‘job’ remains elusive in his account. He talks about military logistics – the ability to ‘fix “the last mile” problem’ – but he also notes the need ‘to fill the basic state functions related to health, security, and public order in order to adequately respond to the threat.’ In case that triptych isn’t clear enough, in his subsequent ‘Ebola Manifesto‘ the major declares that ‘There is exactly one organization designed to rapidly hold and control territory and the people on it: the military.’ The figure he eventually arrives at – somewhere between 36,600 to 73,200 troops – is derived from the wars in Afghanistan and Iraq, and suggests that, for some commentators at least, the Ebola crisis is an opportunity to deepen AFRICOM’s investment in what Jan Bachmann calls ‘policing Africa’ [see his ‘Policing Africa: the US military and visions of crafting “good order”‘, Security Dialogue 45 (2) (2014) 119-36]:
‘The spectrum of [AFRICOM’s] activities can be understood most comprehensively through an analytical perspective of policing, in which the aim of establishing ‘good order’ through an expansive regulatory engagement in issues of welfare is applied to contexts of ‘fragile’ statehood and ‘ungoverned spaces’.’
This is not a uniquely American view. The Daily Mail (where else?) reports that one of the options being considered by Britain’s Chief of the General Staff is a full-scale military lockdown of Sierra Leone:
‘From a military perspective ebola is like a biological warfare attack and should be countered accordingly. There needs to be a clampdown on human movement inside Sierra Leone and possibly to and from the country between now and late 2015 when it is hoped that an antidote will have been developed.’
It’s hard to know how much credence this should be given, of course, though the very existence of proposals like these suggests that the ‘soft power’ which Joeva Rock sees in the militarisation of Ebola conceals an iron fist. And Niles Williamsonbelieves that the military-medical missions are a smokescreen:
‘The main purpose of this military operation is not to halt the spread of Ebola or restore health to those that have been infected. Rather the United States is seeking to exploit the crisis to establish a firm footing on the African continent for AFRICOM.’
That may be one of the objectives, but I think it’s a bridge too far to claim it as the main purpose: as I’ve tried to show, the militarisation and securitisation of Ebola has many other geopolitical and biopolitical dimensions. And Nick Turse has revealed that AFRICOM, far from having a ‘light footprint’, has already achieved a remarkably rapid tempo of operations across the whole continent.
Still, even in its less extreme versions, the ‘war on Ebola’ clearly raises urgent questions about the militarisation of humanitarian aid, about what Kristin Bergtora Sandvikcalls a ‘crisis of humanitarian governance’, and about the violence that is involved in the production of the humanitarian present.
I discussed the History of Violence project’s Disposable Life series when it was first announced here. Introducing the series, the Project’s Director Brad Evansexplains:
“Mass violence is poorly understood if it simply refers to casualties on battlefields or continues to be framed through conventional notions of warfare. We need to interrogate the multiple ways in which entire populations are rendered disposable on a daily basis if we are to take seriously the meaning of global citizenship in the 21st Century”.
Nine videos have been produced so far, and you can access the first eight here; the latest comes from Slavoj Zizek:
For Zizek, the issue of ‘disposable lives’ in the contemporary period does not simply relate to some small or invisible minority. According to the new logics of global capitalism, the vast majority of the worlds citizens (including almost entire Nations) are deemed to be worthless and superfluous to its productive needs. Not only does this point to new forms of apartheid as the global cartography for power seeks to police hierarchies of disposability, it further points to a nihilistic future wherein the aspirations of many are already being sacrificed.
You can access the video through the links above or directly from vimeohere. Not my favourite theorist or commentator, but worth watching not least for the one-liner about Sloterdijk (at 4.06 if you’re really busy). What he takes from Sloterdijk is this:
‘”global” means there is a globe which is not all-encompassing, it’s a globe where from within you think it’s endless, all encompassing, you see it all, but no, it excludes…’
I agree with Brad’s framing of the project – impossible not to, I think – but once you start to imagine the global in these (un)exceptionable terms, both conventional and unconventional modes of warfare start to seep back in to the discussion. For on those now radically dispersed and discontinuous battle spaces whole populations are being rendered disposable on a daily basis.
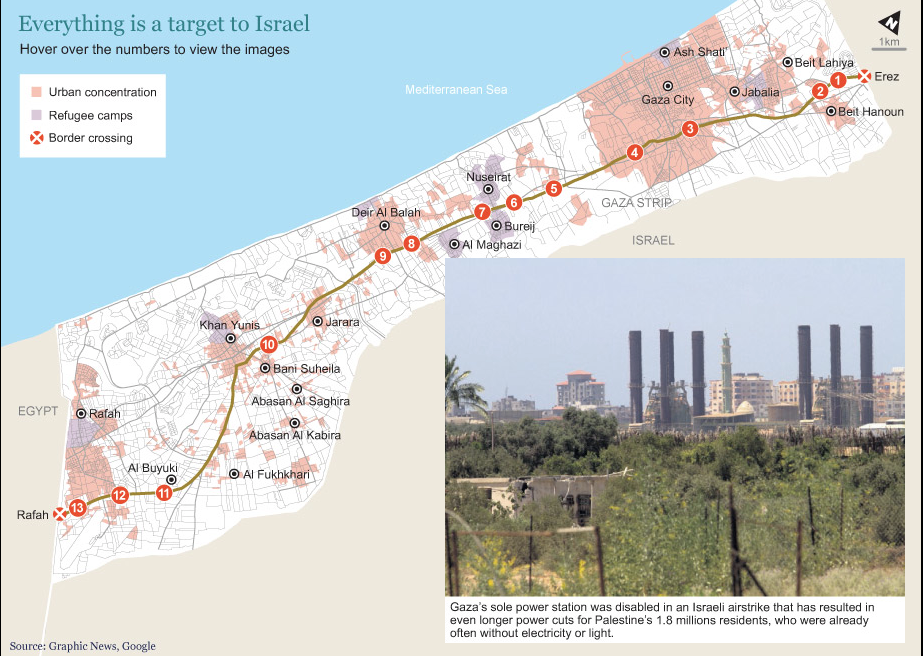
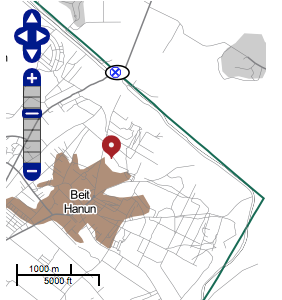
In a previous post on ‘The Death Zone‘, I suggested readers compare Israel’s extended ‘buffer zone’ in Gaza by following the line of the main highway, Saladin Street. Hugh Naylor has followed that route on the ground – what he calls ‘Desolation Road’ – and his report is accompanied by an interactive map showing some of the vast panorama of destruction:
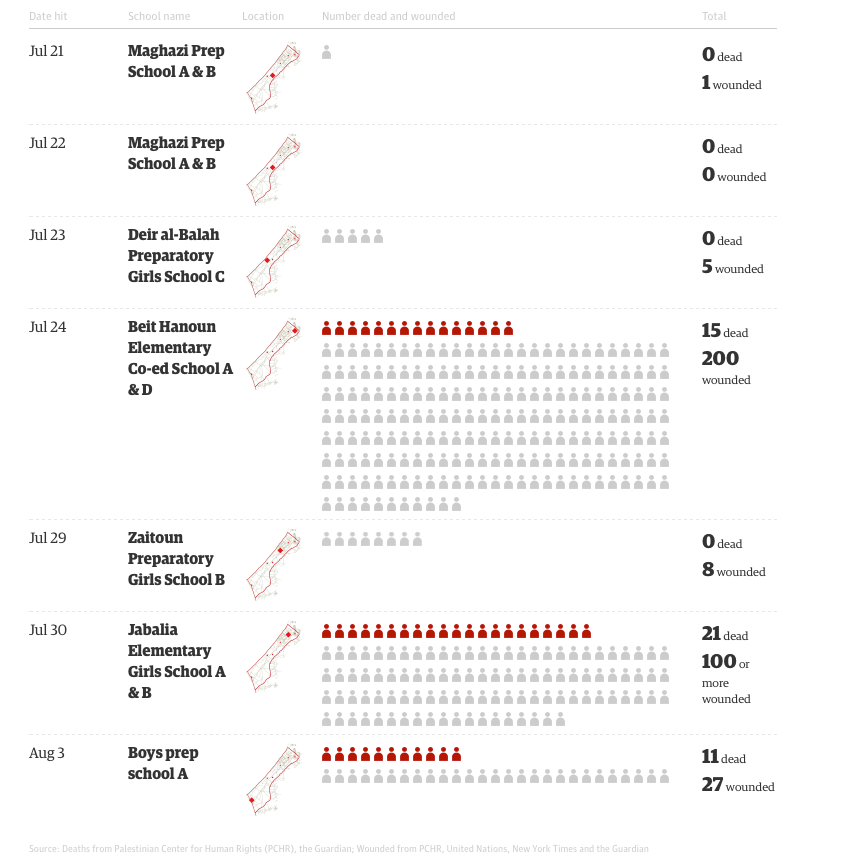
I’ll have more to say about the caption – about the Israeli military’s targeting in Gaza – shortly. The Guardian has just published a graphic by Nadja Popovich showing the UNRWA-run schools sheltering refugees (many of them from the expanded ‘buffer zone’) that were struck by the Israeli military:
Amnesty Internationalreports growing evidence that health facilities and workers were deliberately targeted by the Israeli military:
Testimonies from doctors, nurses, and ambulance workers who have spoken to Amnesty International paint a disturbing picture of hospitals and health professionals coming under attack by the Israeli army in the Gaza Strip, where at least six medics have been killed. There is growing evidence that health facilities or professionals have been targeted in some cases.
Since Israel launched Operation “Protective Edge” on 8 July, the Gaza Strip has been under intensive bombardment from the air, land and sea, severely affecting the civilian population there. As of 5 August, according to the UN Office for the Coordination of Humanitarian Affairs, 1,814 Palestinians had been killed in the Gaza Strip, 86 per cent of them civilians. More than 9,400 people have been injured, many of them seriously. An estimated 485,000 people across the Gaza Strip have been displaced, and many of them are taking refuge in hospitals and schools.
Amnesty International has received reports that the Israeli army has repeatedly fired at clearly marked ambulances with flashing emergency lights and paramedics wearing recognizable fluorescent vests while carrying out their duties. According to the Palestinian Ministry of Health, at least six ambulance workers, and at least 13 other aid workers, have been killed as they attempted to rescue the wounded and collect the dead. At least 49 doctors, nurses and paramedics have been injured by such attacks; at least 33 other aid workers were also injured. At least five hospitals and 34 clinics have been forced to shut down due to damage from Israeli fire or continuing hostilities in the immediate area.
Hospitals across the Gaza Strip suffer from fuel and power shortages (worsened by the Israeli attack on Gaza’s only power plant on 29 July), inadequate water supply, and shortages of essential drugs and medical equipment. The situation was acute before the current hostilities, due to Israel’s seven-year blockade of Gaza, but have been seriously exacerbated since…
Amnesty International is aware of reports that Palestinian armed groups have fired indiscriminate rockets from near hospitals or health facilities, or otherwise used these facilities or areas for military purposes. Amnesty International has not been able to confirm any of these reports. While the use of medical facilities for military purposes is a severe violation of international humanitarian law, hospitals, ambulances and medical facilities are protected and their civilian status must be presumed. Israeli attacks near such facilities – like all other attacks during the hostilities – must comply with all relevant rules of international humanitarian law, including the obligation to distinguish between civilians and civilian objects and military targets, the obligation that attacks must be proportional and the obligation to give effective warning. Hospitals and medical facilities must never be forced to evacuate patients under fire.
The report includes detailed testimony from Palestinian paramedics and ambulance crews who describe the extraordinary difficulty and danger they faced in attending to casualties from Israeli shelling (see also my post on ‘Gaza 101‘, the emergency number for Gaza, and the update here). Not surprisingly, Israel has rejected Amnesty’s claims and denied targeting hospitals, but when Netanyahu’s spokesperson, Mark Regev, explained that ‘What we’ve had to do on a number of occasions is to hit terrorist targets in the immediate vicinity of hospitals and things like that, where they’ve abused them,’ he failed to address the violations of international law summarised in the last paragraph above.
There’s more. B’Tselem, now back on line, is also providing detailed testimony from Gaza, including (so far) two ambulance drivers, Rami ‘Abd al-Haj ‘Ali and Ahmad Sabah. Here is an extract from the first statement (all testimonies are linked to B’Tselem’s interactive map):
On Friday afternoon, 25 July 2014, I was working at the medical emergency call center in Beit Hanoun. At around 4:30 P.M., we received a call reporting injured people in al-Masriyin Street in Beit Hanoun. We asked the International Red Cross to coordinate our going there. About 15 minutes after we received the call, we got authorization and an ambulance headed over there with paramedics ‘Aaed al-Bura’i, 25, Hatem Shahin, 38, and driver Jawad Bdeir, 52. The team didn’t make it to the wounded people. Soon after they reached the street, they reported back that a tank had fired at them and they were injured. They asked for another team to come and rescue them.
The call center coordinated the arrival of another team with the International Red Cross and got authorization to go rescue the injured team. I drove the second ambulance, and there were two medics with me – Muhammad Harb, 31, and Yusri al-Masri, 54. The street is only about 200-300 meters from the call center, so we were there within minutes. When we reached the entrance to the street, we were surprised to see three tanks and a military bulldozer in the street, about 100 meters away.
Suddenly, with no warning, they opened heavy machine-gun fire at us. The bullets penetrated the ambulance. I tried to turn the ambulance around to get out of there, but the steering wheel must have been hit. Suddenly, I felt sharp pain in my leg and realized I’d been hit by a bullet or shrapnel. Then the windshield shattered. Because I couldn’t turn the ambulance around, I decided to try reversing. They kept firing as I backed up, until we got far enough away. When they stopped, I managed to turn us around and head back to the center.
On the way there we met Hatem Shahin, one of the paramedics from the first ambulance. He’d been hit by shrapnel in his shoulder and leg. He told us that a shell fired from a tank had hit the front part of the ambulance. He said he’d managed to get away but the other paramedic, ‘Aaed, had been hit. He told us that after he ran away from there, he saw the tank fire another shell at the ambulance, completely destroying it. He thought ‘Aaed must have been killed, but we didn’t know for sure.
The next day, on Saturday, a ceasefire was declared from 8:00 A.M. to 8:00 P.M. An ambulance team went to the spot and found ‘Aaed’s body in the burnt ambulance.
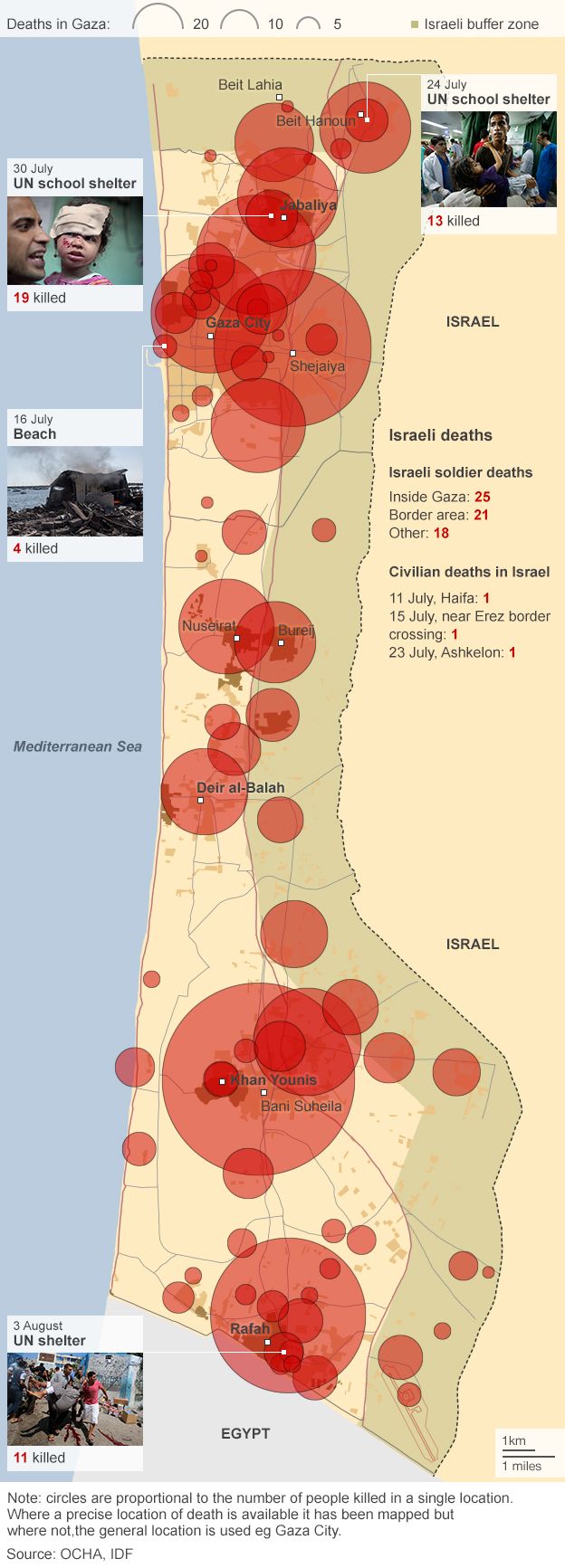
To put all of this in context, the BBC has mapped the deaths of 1,890 Palestinians – ‘mostly civilians’, as its accompanying chart shows – killed during the Israeli offensive to 6 August. As you can see, Palestinians were killed ‘right across Gaza’ – not only in the expanded buffer zone shown on the map, though the carnage in Beit Hanoun and Shejaiya is clearly visible – with high concentrations also produced in the killing grounds of Gaza City and Khan Younis:
Finally, in case you’re puzzled by the title for this post: Israel’s attack on Gaza is codenamed Tzuk Eitan in Hebrew, meaning ‘Firm Cliff’ or ‘Resolute Cliff’. According to Yagiv Levy, ‘The operation’s name signals the power, commitment and resilience of the Israeli people.’ But the official English-language version, ‘Protective Edge’, was changed ‘to give it a more defensive connotation’ (really). As Steven Pooleexplains, ‘the bombing was supposedly “protective”, though not of those bombed’. All of this is of course in line with the designation of the Israeli military as the ‘Israeli Defence Forces’.
I decided I’d prefer to use a version that provides a more accurate rendering of what has happened – in Hebrew, English or Arabic.
We are in the preparatory stages for a new edition of the Dictionary of Human Geography, which I’m co-editing this time with Clive Barnett, Jeremy Crampton, Diana Davis, Geraldine Pratt, Joanne Sharp and Henry Yeung. At the moment, we are making devilishly difficult decisions over headwords (which to cut, which to add) and lengths (which to shorten, which to increase). Of course, none of this is set in stone, and new entries always press themselves forward as the submission deadline draws near. Sometimes they are words you wonder why they weren’t included in the first place.
One such, last time round, was ‘Holocaust’: a glaring omission from previous editions, I belatedly realised. There was, after all, a considerable body of geographical work on it, some of it by geographers, which I did my best to incorporate in the entry I wrote in short order for the last edition. In truth, I suspect I noticed the omission through my interest in Giorgio Agamben‘s Homo sacer and Remnants of Auschwitz; thinking about the geographies of the Holocaust made me realise that the space of the exception, however defined, was not limited by the barbed perimeter of the camp but extended out along the railway tracks to the ghettoes, the round-ups and a host of capillary and diminishing exceptions (see my discussion here). This in turn makes the spatiality of the exception of constitutive significance.
This book explores the geographies of the Holocaust at every scale of human experience, from the European continent to the experiences of individual human bodies. Built on six innovative case studies, it brings together historians and geographers to interrogate the places and spaces of the genocide. The cases encompass the landscapes of particular places (the killing zones in the East, deportations from sites in Italy, the camps of Auschwitz, the ghettos of Budapest) and the intimate spaces of bodies on evacuation marches. Geographies of the Holocaust puts forward models and a research agenda for different ways of visualizing and thinking about the Holocaust by examining the spaces and places where it was enacted and experienced.
1. Geographies of the Holocaust / Alberto Giordano, Anne Kelly Knowles, and Tim Cole
2. Mapping the SS Concentration Camps / Anne Kelly Knowles and Paul B. Jaskot, with Benjamin Perry Blackshear, Michael De Groot, and Alexander Yule
3. Retracing the “Hunt for Jews”: A Spatio-Temporal Analysis of Arrests during the Holocaust in Italy / Alberto Giordano and Anna Holian
4. Killing on the Ground and in the Mind: The Spatialities of Genocide in the East / Waitman W. Beorn, with Anne Kelly Knowles
5. Bringing the Ghetto to the Jew: The Shifting Geography of the Budapest Ghetto / Tim Cole and Alberto Giordano
6. Visualizing the Archive: Building at Auschwitz as a Geographic Problem / Paul B. Jaskot, Anne Kelly Knowles, and Chester Harvey, with Benjamin Perry Blackshear
7. From the Camp to the Road: Representing the Evacuations from Auschwitz, January 1945 / Simone Gigliotti, Marc J. Masurovsky, and Erik Steiner
8. Afterword / Paul B. Jaskot and Tim Cole
Tim Cole is the author of a series of outstanding geographical studies of the Holocaust, including Holocaust City on Budapest; he’s now Professor of Social History at Bristol, but his PhD in Geography at Cambridge was started under the supervision of Graham Smith, one of my dearest friends, who tragically died before the thesis was completed.
Here’s another old Cambridge friend Geoff Eleyon the present collaborative project: ‘As a pioneering call to extend our familiar approaches, Geographies of the Holocaust offers a welcome model of collaborative interdisciplinarity — between historians and geographers, humanities and the social sciences, distinguished specialists and scholars from the outside. The desired purposes are admirably served. Thinking with space delivers not only a new range of challenging methodologies, but brings the well-established findings of the field under strikingly new perspectives too.’
I’ve praised Laleh Khalili‘s Time in the shadows before, and Jadaliyya has now reprinted an excerpt that is of renewed urgency in the face of the Israeli assault on Gaza. Laleh explains:
I wrote Time in the Shadows in order to puzzle out why the counterinsurgency practices of enormously powerful state militaries—the US and Israel at the time I was writing the book—so often invoked law and humanitarianism, rather than naked force. And why so much of their war-fighting pivoted around the mass confinement not only of combatants but civilians. I was also struck by the similarities in the practices of confinement not only between Israel and the US but with historical accounts of colonial confinement effected by Britain and France.
For me, what was striking, insidious, devastating, was the less flashy, less visible, practices that were foundational to detention of suspected combatants and incarceration—whether in situ or through resettlement—of troublesome civilians. These practices—law, administration, demographic and anthropological mapping, offshoring—all sounded so dry, so rational, and yet they were grist to the mill of liberal counterinsurgents in so many ways. And the other similarity across a century and several continents seemed to be the repetition ad nauseam of the language of “protection” and of “security” to frame or rename or euphemise atrocities.
Among the technologies that best embody this language of protection used to violently pacify a population in counterinsurgencies are the separation wall and the various “protective” zones invented by the Israeli military to fragment the Palestinian territories and ensure panopticon-like surveillance and monitoring capability over these fragmented zones. These technologies have specific histories and are mirrored in so many different contexts. The following excerpt is an attempt at situating the wall and the various zones in both a longer historical continuum with colonial practices, while also reflecting on the settler-colonial specificities of their present form.
Laleh describes seam zones, security zones until, finally, she arrives at death zones:
Brigadier General Zvika Fogel, the former head of Southern Command, explained that after the Second Intifada, the Southern Command unofficially declared death zones in Gaza, where anyone entering could be shot: “We understood that in order to reduce the margin of error, we had to create areas in which anyone who entered was considered a terrorist.”
“When you want to use something, you have no problem finding the justification, especially when we hit those we wanted to hit when we used them at the start of the events. If at the beginning we could justify it operationally, then even if there were personnel from the Advocate General’s Office or from the prosecution, it was easy to bend them in the face of the results…
According to the Internal Displacement Monitoring Centre, the Israeli military unilaterally implemented an undefined “no-go” zone inside Gaza in 2000. It started to level lands near the border fence (which had been put in place in 1994), particularly around Rafeh, and ‘by mid-2006 Israel was leveling lands 300 to 500 meters from the fence.’ In 2010 the World Food Programme in collaboration with OCHA produced a report, ‘Between the Fence and a Hard Place‘, documenting the hardships and the horrors and in 2011 Diakonia produced a detailed report on the (il)legal armature of the buffer zone, ‘Within Range‘. It concluded:
The use of force based on military necessity must be engaged in good faith and consistent with other rules of IHL, in particular the principles of distinction and proportionality and precautions in and during attack. This does not appear to be the case in the “buffer zone” as the violations to IHL are flagrant, frequent and grave. Israel remains the Occupying Power in the Gaza Strip. In this capacity, it must protect the safety and well-being of the Palestinian population and take Palestinian needs into account. In addition, Israel must also protect Israeli civilians and soldiers, but it is not allowed to do so at disproportionate expense to Palestinian civilian lives and property.
While acknowledging Israel’s security concerns regarding attacks on Israel from the Gaza Strip, the facts and information available show that the unilateral expansion of the “buffer zone” and its enforcement regime result in violations of international humanitarian law and grave infringement of a number of rights of Palestinians.
In 2012 OCHA estimated that up to 35 per cent of Gaza’s agricultural land had been affected by these restrictions at various times, and the Gazan economy had sustained a loss of around 75,000 MT of agricultural produce each year ($50 million p.a.)
The situation in December 2012 is set out on the map below, which shows what the Israeli military defined as ‘Access Restricted Areas’ (ARA) which, on the landward side, comprised three zones:
(1) A ‘No-Go Zone’, 100 metres wide, which was cleared of all vegetation and all built structures;
(2) A ‘restricted zone’, a further 100-300 metres wide, where access was permitted on foot and for farmers only;
(3) A ‘risk zone’…
You can download a hi-res version here (see also Léopold Lambert‘s maps and commentary here). In practice, the UN Office of the Commissioner for Human Rights explained, ‘the “no go zone’’ on land was at times enforced a few hundred metres beyond this, with a “high risk zone” extending sometimes up to 1,500 metres.’ In November 2012 these restrictions were supposed to be eased, as part of the agreement ending the Israeli offensive earlier that month. But as the Commissioner reported, ‘there has been an increased level of uncertainty regarding the access restrictions imposed on land since this date.’ In the spring UN monitoring teams reported that in most cases farmers could not enter lands within 300 metres of the fence and that the Israeli military fired warning shots if they attempted to do so, that in some places the exclusion zone extended beyond 300 metres, and that there was continued concern about the presence of unexploded ordnance in the border areas. The map produced by Gisha: Legal Center for Freedom and Movement for September 2013, ‘Mapping movement and access‘, reflects these realities, and you can find a detailed report from the Palestinian Center for Human Rights and the IDMC, Under Fire: Israel’s enforcement of access restricted areas in the Gaza Strip (February 2014) here.
Unexploded ordnance is a matter of grave concern, but there has also been a history of live-fire incidents (see the graph below). Since December 2013 and before the current Israeli offensive the number of live-fire casualties near the fence was increasing again. In a ten week period between December 2013 and March 2014 B’Tselem field researcher Muhammad Sabah documented 55 civilians injured near the fence: 43 by live fire; 10 by rubber bullets; and two hit by teargas canisters [I can’t link to the report at the moment because the B’Tselem website is under attack and has been taken off the grid; I can now – it’s here].
These live-fire incidents are sometimes carried out from remote-controlled stations; the system is called ‘Spot and Strike‘. Michael Morpurgo, the creator of “War Horse”, saw its effects when he visited Gaza in November 2010 as a representative of Save the Children:
“I stood in among the ruins watching the kids at work, coming and going with their donkeys and carts. They didn’t seem worried, so I wasn’t worried… I heard the shots, then the screaming, saw the kids running to help their wounded friends. Now I really was outside the comfort zone of fiction. A doctor from Medecins Sans Frontieres told me that the shots were not fired by snipers from the watchtowers on the wall, as I had supposed, but that these scavengers were routinely targeted, electronically from Tel Aviv, which was over 25 kilometres away – ‘Spot and Strike’, the Israelis call it.
“It was like a video game – a virtual shooting, only it wasn’t: there was blood, his trousers were soaked in it, the bullets were real. I saw the boy close to, saw his agony as the cart rushed by me. Many like him, the doctor told me, ended up maimed for life. Here was a child, caged and under siege, being deliberately targeted, his right to survival, the most basic of all children’s rights, being utterly ignored. Unicef says that 26 children were shot like this in 2010. The boy I saw was called Shamekh, I discovered. He lives in a house with 15 family members, and was out there earning what money he could, in the only way he knew how.’
Today, there is a palpable sense in which the whole of Gaza has become a death zone. First, Israel has declared a three-kilometre ‘buffer zone’ inside Gaza’s borders which now effectively places 44 per cent of the territory off limits (you can download the OCHA map below here; the second map makes the situation clearer, though it inevitably sacrifices detail). Compare this with the previous map by following the line of the road south-north.
Léopold Lambert has provided this close-in triptych which exposes the enormity of the expansion and the knock-on effects of the forced displacement:
Anyone within the zone has been warned by the Israeli military to leave or risk being bombed.
This buffer zone has only exacerbated Gaza’s siege. To the east, Palestinians in Gaza are fenced in by Israeli artillery tanks, mortars, cannon shells and snipers. On Gaza’s western side, Israeli warships form a blockade and allow only a three-mile fishing zone. To the north resides more military checkpoints and soldiers. To the south, the Egyptian military has closed off the Rafah border.
The buffer zone has tightened the Israeli chokehold around Gaza’s small strip of land.
This is, as Jesse Rosenfedreports, a ‘No Man’s Land’ in exactly the expanded sense proposed by Noam Leshem and Al Pinkerton:
What that means on the ground is scenes of extraordinary devastation in places like the Al Shajaya district approaching Gaza’s eastern frontier, and Beit Hanoun in the north. These were crowded neighborhoods less than three weeks ago. Now they have been literally depopulated, the residents joining more than 160,000 internally displaced people in refuges and makeshift shelters. Apartment blocks are fields of rubble, and as I move through this hostile landscape the phrase that keeps ringing in my head is “scorched earth.”
It’s not like Israel didn’t plan this. It told tens of thousands of Palestinians to flee so its air force, artillery and tanks could create this uninhabitable no-man’s land of half-standing, burned-out buildings, broken concrete and twisted metal. During a brief humanitarian ceasefire some Gazans were able to come back to get their first glimpse of the destruction this war has brought to their communities, and to sift through their demolished homes to gather clothes or other scattered bits of their past lives. But many were not even able to do that.
Satellite imagery has confirmed the scale of the devastation; the map (right) is based on just three areas within the expanded ‘buffer zone’ and was compiled from imagery taken before the intensification of the onslaught. You can find details of the UNITAR/UNOSAT programme and image files here. If you can bear to get closer, there are photographs taken on the ground here and here.
Second, the Israeli military have not confined their operations to the expanded buffer zone, and those who have – somehow – found sanctuary outside its limits (but of necessity still within the closed and shuttered confines of Gaza) have found that they are pursued by aircraft and tanks. The image below, taken from the same source (and same date) used to compile the map above, shows a wide arc of damage in central Gaza far beyond the ‘zone’ (see also my previous posts here, here and here; you can also find a detailed interactive photo-map of the whole territory from the New York Timeshere).
‘The problem,’as one young resident explained to Anne Barnard, ‘is that when we are fleeing from the shelling, we still find the shelling around us.’ Stories abound of families seeking refuge only to find death waiting for them. One man toldAlexandra Zavis that his brother, four sisters, brother-in-law and five young children escaped from eastern Gaza to what they thought was a safe place in central Gaza City, only to be killed when the top floors of the building collapsed after an Israeli air strike the very next day. Others tell similar stories – one family moving twice before eventually ten of them were killed. And then there are all those who have sought refugee in UNRWA camps, many of them schools, or who have been rushed to hospitals for treatment, only to be bombed and shelled there too.
Ha’aretz‘s headline on 31 July says it all: ‘The Gaza battlefield is crowded with the displaced and the homeless.’ So it is. And still they are bombed and shelled. As UNRWA’s Chris Gunness put it, ‘Gaza is unique in the annals of modern warfare in being a conflict zone with a fence around it, so civilians have no place to flee.’
In his seminal essay on ‘Necropolitics‘, written more than ten years ago, Achille Mbembe had this to say:
Late-modern colonial occupation differs in many ways from early-modern occupation, particularly in its combining of the disciplinary, the biopolitical, and the necropolitical. The most accomplished form of necropower is the contemporary colonial occupation of Palestine…
Entire populations are the target of the sovereign. The besieged villages and towns are sealed off and cut off from the world. Daily life is militarized… The besieged population is deprived of their means of income. Invisible killing is added to outright executions…
I have put forward the notion of necropolitics and necro-power to account for the various ways in which, in our contemporary world, weapons are deployed in the interest of maximum destruction of persons and the creation of death-worlds, new and unique forms of social existence in which vast populations are subjected to conditions of life conferring upon them the status of living dead.
Gaza has been systematically turned not only into a prison, then, but also into a camp: and the lives of those within have been have been subjected to a ruthless bio-political programme that, at the limit, has become a calculated exercise in necro-politics. This confirms Paul Di Stefano‘s claim that that, for the Israeli military, Gaza has been transformed into ‘a state of exception where normal rights do not apply. Within this liminal space, Palestinian bodies are viewed as obstacles to be destroyed or controlled in the maintenance of the colonial order.’
101 is the emergency number for Gaza and the rest of occupied Palestine. And perhaps I should begin with that sentence: I say ‘the rest of occupied Palestine’ because, despite Israel’s ‘disengagement’ from Gaza in 2005, Israel continues to exercise effective control over the territory which means that Gaza has continued to remain under occupation. It’s a contentious issue – like Israel’s duplicitous claim that the West Bank is not ‘occupied’ either (even by its illegal settlers) merely ‘disputed’ – and if you want the official Israeli argument you can find it in this short contribution by a former head of the IDF’s International Law Department here and here. The value of that essay – apart from illustrating exactly what is meant by chutzpah – is its crisp explanation of why the issue matters:
‘This does not necessarily mean that Israel has no legal obligations towards the population of the Gaza Strip, but that to the extent that there are any such legal obligations, they are limited in nature and do not include the duty to actively ensure normal life for the civilian population, as would be required by the law of belligerent occupation…’
Certainly, one of the objectives of Israel’s ‘disengagement’ was to produce what its political and military apparatus saw as ‘an optimal balance between maximum control over the territory and minimum responsibility for its non-Jewish population’. That concise formulation is Darryl Li‘s, which you can find in his excellent explication of Israel’s (de)construction of Gaza as a ‘laboratory’ for its brutal bio-political and necro-political experimentations [Journal of Palestine Studies 35 (2) (2006)]. (Another objective was to freeze the so-called ‘peace process’, as Mouin Rabbaniexplains in the latest London Review of Bookshere; his essay also provides an excellent background to the immediate precipitates of the present invasion). Still, none of this entitles Israel to evade the obligations of international law. Here it’s necessary to recall Daniel Reisner‘s proud claim that ‘If you do something for long enough, the world will accept it… International law progresses through violations’: Reisner also once served as head of the IDF’s International Law Department, and the mantra remains an article of faith that guides IDF operations. But as B’Tselem, the Israeli Information Center for Human Rights in the Occupied Territories, insisted in an important opinion published at the start of this year:
Even after the disengagement, Israel continues to bear legal responsibility for the consequences of its actions and omissions concerning residents of the Gaza Strip. This responsibility is unrelated to the question of whether Israel continues to be the occupier of the Gaza Strip.
But there’s more. International humanitarian law – no deus ex machina, to be sure, and far from above the fray – not only applies during Israel’s military offensives and operations, including the present catastrophic assault on Gaza, but provides an enduring set of obligations. For as Lisa Hajjar shows in a detailed discussion re-published by Jadaliyya last week, Israel’s attempts to make Gaza into a space of exception – ‘neither sovereign nor occupied’ but sui generis – run foul of the inconvenient fact that Gaza remains under occupation. Israel continues to control Gaza’s airspace and airwaves, its maritime border and its land borders, and determines what (and who) is allowed in or out [see my previous post and map here]. As Richard Falkargues, ‘the entrapment of the Gaza population within closed borders is part of a deliberate Israeli pattern of prolonged collective punishment’ – ‘a grave breach of Article 33 of the Fourth Geneva Convention’ – and one in which the military regime ruling Egypt is now an active and willing accomplice.
So: Gaza 101. Medical equipment and supplies are exempt from the blockade and are allowed through the Karam Abu Salem crossing (after protracted and expensive security checks) but the siege economy of Gaza has been so cruelly and deliberately weakened by Israel that it has been extremely difficult for authorities to pay for them. Their precarious financial position is made worse by direct Israeli intervention in the supply of pharmaceuticals. Corporate Watch reports that
When health services in Gaza purchase drugs from the international market they come into Israel through the port of Ashdod but are not permitted to travel the 35km to Karam Abu Salem directly. Instead they are transported to the Bitunia checkpoint into the West Bank and stored in Ramallah, where a permit is applied for to transport them to Gaza, significantly increasing the length and expense of the journey.
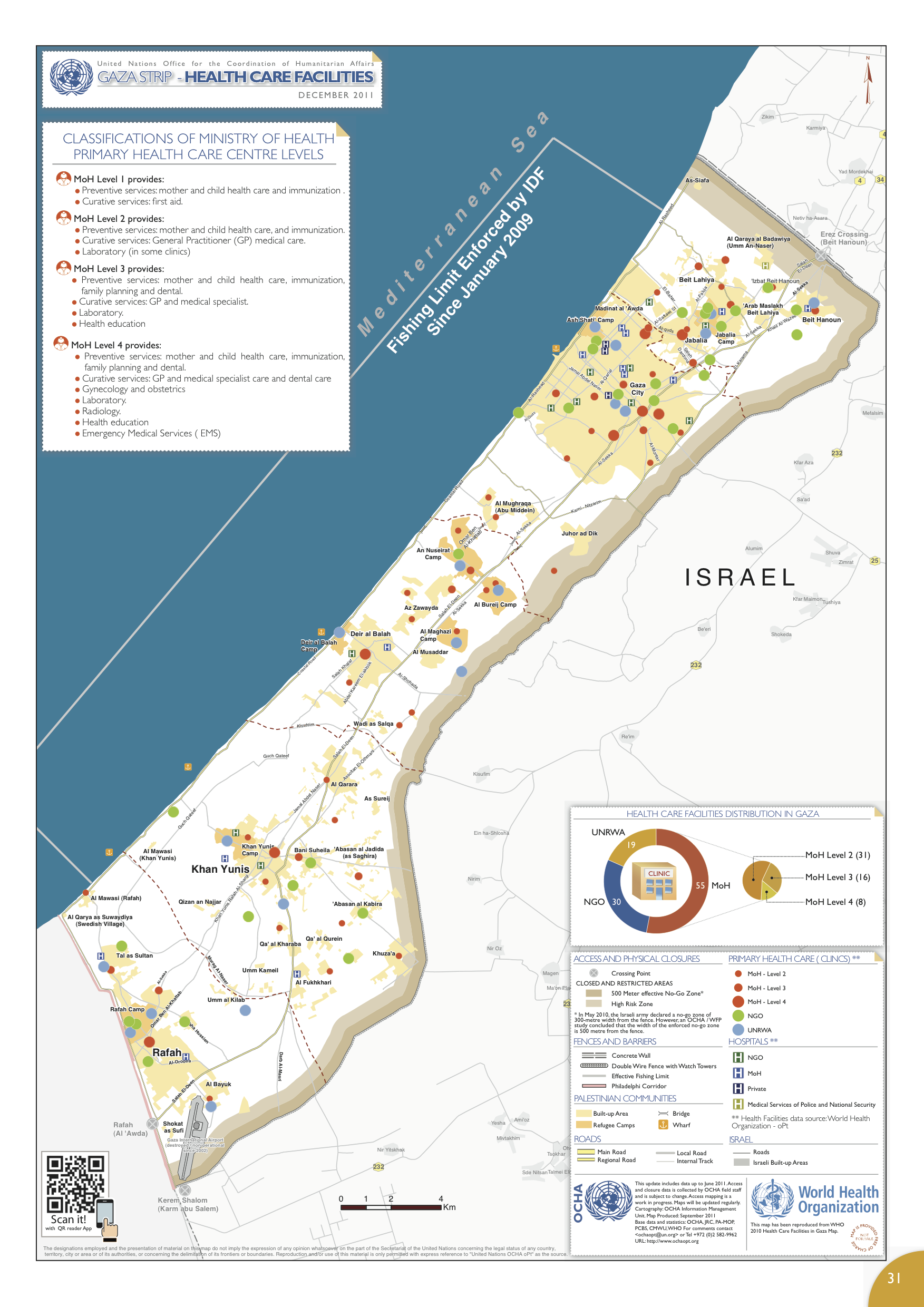
There’s more – much more: you can download the briefing here – but all this explains why Gaza depends so much on humanitarian aid (and, in the past, on medical supplies smuggled in through the tunnels). Earlier this summer Gaza’s medical facilities were facing major shortfalls; 28 per cent of essential drugs and 54 per cent of medical disposables were at zero stock.
Medical care involves more than bringing in vital supplies and maintaining infrastructure (the map of medical facilities above is taken from the UN’s humanitarian atlas and shows the situation in December 2011; the WHO’s summary of the situation in 2012 is here). Medical care also involves unrestricted access to electricity and clean water; both are compromised in Gaza, and on 1 January 2014 B’Tselem reported a grave deterioration in health care as a result:
‘The siege that Israel has imposed on the Gaza Strip since Hamas took over control of the security apparatus there in June 2007 has greatly harmed Gaza’s health system, which had not functioned well beforehand…. The reduction, and sometimes total stoppage, of the supply of fuel to Gaza for days at a time has led to a decrease in the quality of medical services, reduced use of ambulances, and serious harm to elements needed for proper health, such as clean drinking water and regular removal of solid waste. Currently, some 30 percent of the Gaza Strip’s residents do not receive water on a regular basis.’
In-bound transfers are tightly constrained, but so too are out-bound movements. Seriously ill patients requiring advanced treatment had their access to specialists and hospitals outside Gaza restricted:
‘Israel has cut back on issuing permits to enter the country for the hundreds of patients each month who need immediate life-saving treatment and urgent, advanced treatment unavailable in Gaza. The only crossing open to patients is Erez Crossing, through which Israel allows some of these patients to cross to go to hospitals inside Israel [principally in East Jerusalem], and to treatment facilities in the West Bank, Egypt, and Jordan. Some patients not allowed to cross have referrals to Israeli hospitals or other hospitals. Since Hamas took over control of the Gaza Strip, the number of patients forbidden to leave Gaza “for security reasons” has steadily increased.’
As in the West Bank, Israel has established a labyrinthine system to regulate and limit the mobility of Palestinians even for medical treatment. Last month the World Health Organization explained the system and its consequences (you can find a detailed report with case studies here):
‘In Gaza, patients must submit a permit application at least 10 days in advance of their hospital appointment to allow for Israeli processing. Documents are reviewed first by the health coordinator but final decisions are made by security officials. Permits can be denied for reasons of security, without explanation; decisions are often delayed. In 2013, 40 patients were denied and 1,616 were delayed travel through Erez crossing to access hospitals in East Jerusalem, Israel, the West Bank and Jordan past the time of their scheduled appointment. If a patient loses an appointment they must begin the application process again. Delays interrupt the continuity of medical care and can result in deterioration of patient health.Companions (mandatory for children) must also apply for permits. A parent accompanying a child is sometimes denied a permit, and often both parents, and the family must arrange for a substitute, a process which delays the child’s treatment.’
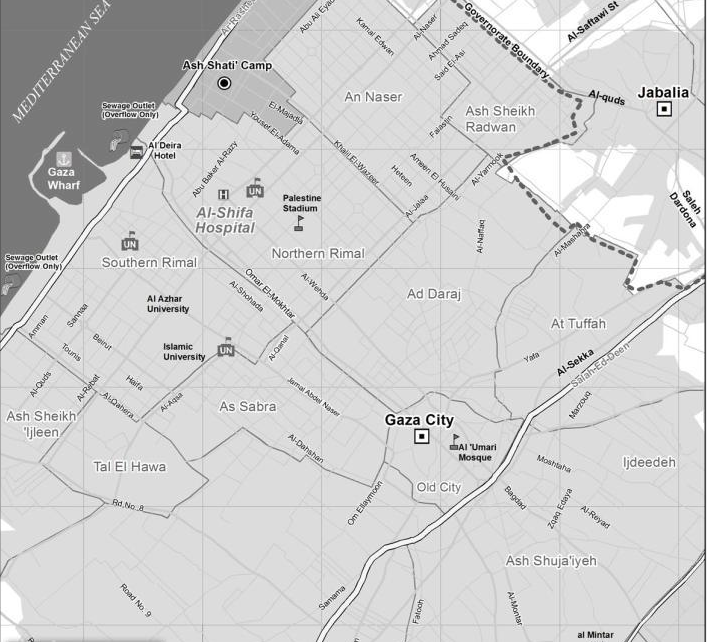
On 17 June Al-Shifa Hospital, the main medical facility in Gaza City (see map below), had already been forced to cancel all elective surgeries and concentrate on emergency treatment. On 3 July it had to restrict treatment to life-saving emergency surgery to conserve its dwindling supplies. All of this, remember, was before the latest Israeli offensive. People have not stopped getting sick or needing urgent treatment for chronic conditions, so the situation has deteriorated dramatically. The care of these patients has been further compromised by the new, desperately urgent imperative to prioritise the treatment of those suffering life-threatening injuries from Israel’s military violence.
Trauma surgeons emphasise the importance of the ‘golden hour’: the need to provide advanced medical care within 60 minutes of being injured. Before the IDF launched its ground invasion, there were three main sources of injury: blast wounds from missiles, penetrating wounds from artillery grenades and compression injuries from buildings collapsing. But this is only a typology; many patients have multiple injuries. ‘We are not just getting patients with one injury that needs attending,’ said the head of surgery at Al-Shifa, ‘we are getting a patient with his brain coming out of his skull, his chest crushed, and his limbs missing.’ All of these injuries are time-critical and require rapid intervention. And yet the Ministry of Health reckons that Gaza’s ambulance service is running at 50 per cent capacity as a result of fuel shortages. That figure must have been reduced still further by the number of ambulances that have been hit by Israeli fire (for more on paramedics in Gaza, and the extraordinary risks they run making 20-30 trips or more every day, see here and this report from the Telegraph‘s David Blair here). When CNN reporters visited the dispatch centre at Jerusalem Hospital in Gaza City last Tuesday, they watched a a screen with illuminated numbers recording 193 killed and 1,481 injured and the director of emergency services dispatching available ambulances to the site of the latest air strike (by then, there had already been over 1,000 of them). But the system only works effectively when there is electricity…
Power supplies were spasmodic at the best of times (whenever those were); they have been even more seriously disrupted by the air campaign, and since the start of the ground assault Gaza has lost around 90 per cent of its power generating capacity. Nasouh Nazzalreports that many hospitals have been forced to switch to out-dated generators to light buildings and power equipment:
“The power generators in Gaza hospitals are not trusted at all and they can go down any moment. If power goes out, medical services will be basically terminated,” [Dr Nasser Al Qaedrah] said. He stressed that the old-fashioned types of power generators available in Gaza consume huge quantities of diesel, a rare product in the coastal enclave.
On occasion, Norwegian ER surgeon Mads Gilberttold reporters, if the lights go out in the middle of an operation ‘[surgeons] pick up their phones, and they use the light from the screen to illuminate the operation field.’ (He had brought head-lamps with him from Bergen but found they were on Israel’s banned list of ‘dual-use’ goods). As the number of casualties rises, the vast majority of them civilians, so hospitals have been stretched to the limit and beyond. According to Jessica Purkiss, the situation was already desperate a week ago:
“The number of injuries is huge compared to the hospitals’ capacity,” said Fikr Shalltoot, the Gaza program director for Medical Aid for Palestinians, an organization desperately trying to raise funds to procure more supplies. “There are 1,000 hospital beds in the whole of Gaza. An average of 200 injuries are coming to them every day.”
As in so many other contemporary conflicts – Iraq, Libya, Syria – hospitals themselves had already become targets for military violence. For eleven days Al-Wafa Hospital in Shuja’iyeh in eastern Gaza City (see the map above), the only rehabilitation centre serving the occupied territories, was receiving phone calls from the IDF warning them that the building was about to be bombed. [In case you’re impressed by the consideration, think about Paul Woodward‘s observation: ‘I grew up in Britain during the era when the Provisional IRA was conducting a bombing campaign in Northern Ireland and on the mainland. I don’t remember the Provos ever being praised for the fact that they would typically phone the police to issue a warning before their bombs detonated. No one ever dubbed them the most humane terrorist organization in the world.’] The staff refused to evacuate the hospital because their patients were paralysed or unconscious. The Executive Director, Dr Basman Alashi, explained:
‘We’ve been in this place since 1996. We are known to the Israeli government. We are known to the Israeli Health Center and Health Ministry. They have transferred several patients to our hospital for rehabilitations. And we have many success stories of people come for rehabilitation. They come crawling or in a wheelchair; they go out of the hospital walking, and they go back to Israel saying that al-Wafa has done miracle to them. So we are known to them, who we are, what we are. And we are not too far from their border. Our building is not too small. It’s big. It’s about 2,000 square meters. If I stand on the window, I can see the Israelis, and they can see me. So we are not hiding anything in the building. They can see me, and I can see them. And we’ve been here for the last 12 or 15 years, neighbors, next to each other. We have not done any harm to anybody, but we try to save life, to give life, to better life to either an Arab Palestinian or an Israeli Jew.’
But just after 9 p.m. on 17 July shells started falling:
‘… the fourth floor, third floor, second floor. Smoke, fire, dust all over. We lost electricity… luckily, nobody got hurt. Only burning building, smoke inside, dust, ceiling falling, wall broke, electricity cutoff, water is leaking everywhere. So, the hospital became [uninhabitable].’
Seventeen patients were evacuated and transferred to the Sahaba Medical Complex in Gaza City. Sharif Abdel Kouddostakes up the story:
‘The electricity went out, all the windows shattered, the hospital was full of dust, we couldn’t see anything,’ says Aya Abdan, a 16-year-old patient at the hospital who is paraplegic and has cancer in her spinal cord. She is one of the few who can speak.
It is, of course, literally unspeakable. But this was not an isolated incident – still less ‘a mistake’ – and other hospitals have been bombed or shelled. According to the Ministry of Health, 25 health facilities in Gaza have been partially or totally destroyed. Just this morning it was reported that Israeli tanks shelled the al-Aqsa Hospital in Deir al-Balah in central Gaza, killing five and injuring 70 staff and patients. The Guardianreports that ambulances which tried to evacuate patients were forced to turn back by continued shelling. According to Peter Beaumont:
‘”People can’t believe this is happening – that a medical hospital was shelled without the briefest warning. It was already full with patients,” said Fikr Shalltoot, director of programmes at Medical Aid for Palestinians in Gaza city.’
The hospitals that remain in operation are overwhelmed, with doctors making heart-wrenching decisions about who to treat and who to send away, refusing ‘moderately injured patients they normally would have admitted in order to make room for the more seriously wounded.’ Mads Gilbert (centre in the image above) again:
Oh NO! not one more load of tens of maimed and bleeding, we still have lakes of blood on the floor in the ER, piles of dripping, blood-soaked bandages to clear out – oh – the cleaners, everywhere, swiftly shovelling the blood and discarded tissues, hair, clothes,cannulas – the leftovers from death – all taken away…to be prepared again, to be repeated all over. More then 100 cases came to Shifa last 24 hrs. enough for a large well trained hospital with everything, but here – almost nothing: electricity, water, disposables, drugs, OR-tables, instruments, monitors – all rusted and as if taken from museums of yesterdays hospitals.
Al-Shifa, where he is working round the clock, has only 11 beds in its ER and just six Operating Rooms. On Saturday night, when the Israeli army devastated the suburb of Shuja’ieyh, its ‘tank shells falling like hot raindrops‘, al-Shifa had to deal with more than 400 injured patients. Al-Shifa is Gaza’s main trauma centre but in other sense Gaza’s trauma is not ‘centred’ at all but is everywhere within its iron walls. Commentators repeatedly describe Gaza as the world’s largest open-air prison – though, given the cruelly calculated deprivation of the means of normal life, concentration camp would be more accurate – but it is also one where the guards routinely kill, wound and hurt the prisoners. The medical geography I’ve sketched here is another way of reading Israel’s bloody ‘map of pain‘. I am sickened by the endless calls for ‘balance’, for ‘both sides’ to do x and y and z, as though this is something other than a desperately unequal struggle: as though every day, month and year the Palestinians have not been losing their land, their lives and their liberties to a brutal, calculating and manipulative occupier. I started this post with an image of a Palestinian ambulance; the photograph below was taken in Shuja’ieyh at the weekend. It too is an image of a Palestinian ambulance.
For updates see here; I fear there will be more to come. In addition to the links in the post above, this short post is also relevant (I’ve received an e-mail asking me if I realised what the initial letters spelled…. Duh.)
James Bridle‘s new installation, Homo Sacer, has opened at FACT (Foundation for Art and Creative Technology) in Liverpool, as part of its Science Fiction: New Death exhibition:
Explore how our relationship with technology has blurred the lines between the real and the virtual; making our everyday lives feel increasingly like science fiction. Artists including James Bridle, Jon Rafman, Mark Leckey, Larissa Sansour and Ryan Trecartin, plus award-winning science fiction author China Miéville present works which explore how technology is creating new ways of living (and dying), of fashioning identities and the growth of cult-like communities.
The exhibition runs until 22 June, and you can (at least virtually) walk through it with Reginehere.
There’s not much detail or documentation of Homo Sacer yet – though see the image above – but James promises a video clip soon. Meanwhile he explains:
The installation consists of a projected “hologram” in the entranceway to the gallery, of the kind increasingly found in airports, railway stations and government buildings. The hologram speaks lines from UK, EU and UN legislation, as well as quotations from government ministers, regarding the nature of citizenship in the 21st century, and how it can be revoked, which potentially fatal consequences.
Other artists have been inspired by Giorgio Agamben‘s discussion(s) of Homo Sacer too (and, for those who take the Latin stubbornly literally, Femina Sacra), of life knowingly and deliberately exposed to death. (If you want an artful preview of the final volume in Agamben’s series, The use of bodies, you can read Adam Kotsko‘s ‘What is to be done? The endgame of the Homo Sacer series’ here.) But back to art. There’s Ben Young‘s Homo Sacer (above), for example, philosopher-artist Adolfo Vásquez Rocca‘s Homo Sacer(below), and and Tarek Tuma‘s haunting Homo Sacer series of canvases showing the faces of suffering in Syria (see here and here), which almost viscerally captures the double meaning of ‘sacra’, sacred and accursed.
In a related vein, as I noted previously, there’s the State of Exception installation which showed what undocumented migrants abandoned as they crossed the US-Mexico border; first staged at the University of Michigan’s Institute for the Humanities, it’s currently at Detroit’s Museum of Contemporary Art. (The wall of backpacks conjures up an after-image of the suitcases on display at Auschwitz, and although they gesture in different directions – one where movement comes to a hideous full stop and the other where flight takes off – both are redolent of Agamben’s preoccupations). For a more wide-ranging view of States of Exception, see Angel Calabres‘s much earlier collaboration here, which trades on Agamben’s work to explore prison subjugation, torture and slaughter houses…
And this in turn brings me (back) to Abdelali Dahrouch‘s installation, Homo Sacer (2009) (below), which is a meditation on the waterboarding of ‘enemy combatants’ by the CIA:
Agamben’s work has inspired not only visual artists. There’s Christoph Winkler‘s dance-work Homo Sacer,for example,now ten years old, which tanzjournal described like this:
The choreographer has truly succeeded in formulating a position that is both an aesthetic and ethical one. Life may be a sacred possession – in the face of sanctioned (war) crimes it becomes a disposable commodity. Dance cannot intervene in this state of affairs. But it can champion life, by displaying it in its vulnerability. Homo Sacer is not only in this respect Winkler’s most impressive piece to date.
And Frankfurter Rundschau like this:
One after another, the other seven dancers climb out of the resting niches. All look distraught in the glaringly lit space, whose angularity contrasts with the fragile bodies. Following abrupt impulses, the dancers break out of themselves, only to quickly fall back into the frozen pose. Humans fleeing and hesitating in the same moment, developing an icy atmosphere of vulnerability … But in the following choreographic sequence, in which the dancers seem to be wrestling with themselves as if the truth were strangling them in its grasp, is a brilliant scene in which the ensemble intertwines and connects into complex structures that, only moments later are again severed. Energy shoots up like suddenly occurring memories – symbolizing the sudden convulsion of that very “base existence”…
And there’s even music – although Martin Kücher released only 250 copies of his solo jazz album Homo Sacer… You can also listen to Vancouver’s own Dubstawk‘s remix Homo Sacerhere.
All sorts of artworks have been used on the cover of Agamben’s texts, of course, and they can be revealing too: I know it’s often wrong to judge a book by its cover (but not always), and my favourite essay in Geographical imaginations is in fact my reading of the cover of David Harvey‘s The condition of postmodernity. In any case, it’s interesting to track movements in the other direction and to see how artists engage with texts – particularly if you believe that artwork is part of the research/investigative/analytical process rather than merely one of its products.
The US military’s obsession with biometrics is, in part, the product of its phantasmatic desire to make the battlespace fully transparent, as its incorporation within the targeting cycle makes clear:
But it’s also a vital means of furthering the profoundly biopolitical project embedded in later modern war (something that intersects, in various ways, with Mark Neocleous‘s arguments about military violence – war power/police power – and ‘ordering’):
The stated goal of the Afghan effort is no less than the collection of biometric data for every living person in Afghanistan. At a conference with Afghan officials in 2010, the commander of the U.S. Army’s Task Force Biometrics Col. Craig Osborne told the attendees that the collection of biometric data is not simply about “identifying terrorists and criminals,” but that “it can be used to enable progress in society and has countless applications for the provision of services to the citizens of Afghanistan.”
I touched on some of this in a different context in ‘The biopolitics of Baghdad’ DOWNLOADS tab), and Public Intelligence has just released the U.S. Army Commander’s Guide to Biometrics in Afghanistan, from which I’ve taken the image above, and which provides a much more detailed accounting.
In a section titled “Population Management,” the U.S. Army’s guide recommends that “every person who lives within an operational area should be identified and fully biometrically enrolled with facial photos, iris scans, and all ten fingerprints (if present).” The soldiers must also record “good contextual data” about the individual such as “where they live, what they do, and to which tribe or clan they belong.” According to the guide, popuation management actions “can also have the effect of building good relationships and rapport” by sending the message that the “census” is intended to protect them from “the influence of outsiders and will give them a chance to more easily identify troublemakers in their midst.”
For a wider, wonderfully critical commentary on biometric war, see Colleen Bell, ‘Grey’s Anatomy goes South: Global racism and suspect identities in the colonial present’, in the Canadian journal of sociology 38 (4) (2013) 465-486 available open access here.

 In what now seems another life, I wrote about US torture during the early years of the “war on terror”, in ‘The Black Flag’ (which was specifically about Guantanamo, and which opened with three ‘suicides’ that we now have good reason to believe were anything but: see here and here) and ‘Vanishing Points’ (which extended the argument to Abu Ghraib and the archipelago of black sites like the ‘Salt Pit’ [shown below] within the global war prison). Both are available in their original forms under the DOWNLOADS tab, and form part of the material I’ve been working with for a new essay to be included in The everywhere war.
In what now seems another life, I wrote about US torture during the early years of the “war on terror”, in ‘The Black Flag’ (which was specifically about Guantanamo, and which opened with three ‘suicides’ that we now have good reason to believe were anything but: see here and here) and ‘Vanishing Points’ (which extended the argument to Abu Ghraib and the archipelago of black sites like the ‘Salt Pit’ [shown below] within the global war prison). Both are available in their original forms under the DOWNLOADS tab, and form part of the material I’ve been working with for a new essay to be included in The everywhere war.
 Now I’m digesting the Executive Summary that has been released by the Senate Select Committee on Intelligence on the CIA’s Detention and Interrogation Program, but you can download the original (redacted) summary here, ‘Other Views’ here, and the Minority View from the Republicans – and please God it remains a minority view – here.
Now I’m digesting the Executive Summary that has been released by the Senate Select Committee on Intelligence on the CIA’s Detention and Interrogation Program, but you can download the original (redacted) summary here, ‘Other Views’ here, and the Minority View from the Republicans – and please God it remains a minority view – here.