This is the third in a new series of posts on military violence against hospitals and medical personnel in conflict zones. It examines some of the key issues arising from the US attack on the Trauma Centre run by Médecins Sans Frontières (MSF) in Kunduz on 3 October 2015; it follows directly from my detailed analysis of the attack here and prepares the ground for a still more detailed analysis of attacks on hospitals, doctors and casualties in Syria to follow.
There are at least four main issues arising from the US attack on the MSF Trauma Centre in Kunduz that spiral out into a wider argument about what I will later call ‘The Death of the Clinic’. I’m treating ‘the clinic’ here as a topological figure that extends from the body of the wounded through the evacuation chain to the hospital itself. The clinic has been accorded a privileged status within the space of exception that is the modern conflict zone – a complicated, fractured space in which killing is made permissible subject to the protocols of international humanitarian law – so that the clinic becomes an exception to the exception and its inhabitants granted a conditional immunity from attack.

It’s important to understand that this legal armature is not immutable, and that changes (and challenges) to it arise through both (geo)political and military actions; international humanitarian law is not a deus ex machina, somehow above the fray, but is thoroughly entangled with the prosecution of military violence. More on this to come, but for now it will be enough to list some of the major protections accorded to the clinic in war-time.
The first Geneva Convention (1864) (‘the Red Cross Convention’):
Ambulances and military hospitals shall be acknowledged to be neuter, and, as such, shall be protected and respected by belligerents so long as any sick or wounded may be therein. Such neutrality shall cease if the ambulances or hospitals should be held by a military force … A distinctive and uniform flag shall be adopted for hospitals, ambulances and evacuations.
Under the Hague Regulations (1899/1907) that were in force during the hospital raids in France at the end of the First World War:
… all necessary steps must be taken to spare, as far as possible, … hospitals, and places where the sick and wounded are collected, provided they are not being used at the time for military purposes. It is the duty of the besieged to indicate the presence of such buildings or places by distinctive and visible signs, which shall be notified to the enemy beforehand.
 Under the Geneva Conventions (1949) – whose provisions applied to the attack on the MSF Trauma Centre a hundred years later – there is a similar immunity granted to the military-medical machine:
Under the Geneva Conventions (1949) – whose provisions applied to the attack on the MSF Trauma Centre a hundred years later – there is a similar immunity granted to the military-medical machine:
The protection to which fixed establishments and mobile medical units of the Medical Service are entitled shall not cease unless they are used to commit, outside their humanitarian duties, acts harmful to the enemy. Protection may, however, cease only after a due warning has been given, naming, in all appropriate cases, a reasonable time limit and after such warning has remained unheeded.
And this is explicitly extended beyond the military-medical machine to institutions like the MSF Trauma Centre:
Civilian hospitals organized to give care to the wounded and sick, the infirm and maternity cases, may in no circumstances be the object of attack but shall at all times be respected and protected by the Parties to the conflict.
The protection to which civilian hospitals are entitled shall not cease unless they are used to commit, outside their humanitarian duties, acts harmful to the enemy. Protection may, however, cease only after due warning has been given, naming, in all appropriate cases, a reasonable time limit and after such warning has remained unheeded.
In so doing the treatment of hostile combatants is also explicitly provided for and protected:
The fact that sick or wounded members of the armed forces are nursed in these hospitals, or the presence of small arms and ammunition taken from such combatants and not yet been handed to the proper service, shall not be considered to be acts harmful to the enemy.
The language and specifications change, but there is nevertheless a consistent thread running through these provisions. It has been stretched – and perhaps broken – by the attack on the MSF Trauma Centre, and here I’ll focus on four issues that have proved contentious. First, the visual identification of the Trauma Centre; second, the alleged breach of its conditional immunity; third, the construal of the attack as a war crime; and fourth, the putative rejection of medical neutrality altogether.
(1) Visual identification
International humanitarian law (IHL) requires those responsible for hospitals ‘to indicate their presence’ – the language varies – in order to ensure their protection, and here the US military investigation made this finding (all page numbers in brackets refer to the redacted report):
The center roof of the MSF Trauma Center was marked with two rectangular MSF flags… The front and sides of the MSF hospital were marked from the street view and a MSF flag flew in the courtyard. The MSF Trauma Center was not marked with any internationally recognized symbols such as a red cross, red crescent or a red “H”. If it had been marked with these symbols, it is possible the Trauma Center would not have been engaged. (082)
This counterfactual does not loom large in the report or its recommendations, but Charles Dunlap (at Lawfire) has seized upon it to berate MSF:
Ask yourself: wasn’t it a mistake for [MSF] – and a serious one – not to have marked its facility in accordance with Protocol III to the Geneva Conventions which designates “the only emblems recognized by nations signifying the protected status of individuals or objects bearing them during armed conflict”? Had, for example, the hospital been marked with large Red Crosses/Red Crescents or one of the other internationally-recognized symbols (as the U.S. does) or something that would make its protected use clear from the air, isn’t it entirely plausible that the aircrew (or someone) might have recognized the error and stopped the attack before it began?
Put another way, isn’t it foreseeable that in an exceptionally chaotic combat situation (where a belligerent is making use of civilian buildings to conduct combat operations) that mistakes could occur in identifying a protected structure absent Protocol III markings or at least something to make it identifiable at a distance, especially when it’s known that attacking aircraft are being used? Wouldn’t reasonably prudent persons have marked their medical facility with an internationally-recognized symbol or something of similar clarity to the warring parties? Wouldn’t due care demand it in that situation?
In accusing MSF of ‘imprudence’ and even recklessness Dunlap applies a double standard. He repeatedly insists that the US and the Afghan militaries confronted ‘an extraordinarily intense situation’ in Kunduz, that they faced ‘terrible urgency’ and ‘enormous pressure’ as they operated ‘in the turmoil of a war zone’ – all of which is undoubtedly true – but he uses this to excuse their mistakes while refusing to extend the same privilege to MSF.

Let me remind you of Dr Kathleen Thomas‘s account of working in the ER (above) once the city had fallen to the Taliban:
The first day was chaos – more than 130 patients poured through our doors in only a few hours. Despite the heroic efforts of all the staff, we were completely overwhelmed. Most patients were civilians, but some were wounded combatants from both sides of the conflict. When I reflect on that day now, what I remember is the smell of blood that permeated through the emergency room, the touch of desperate people pulling at my clothes to get my attention begging me to help their injured loved ones, the wailing, despair and anguish of parents of yet another child lethally injured by a stray bullet whom we could not save, my own sense of panic as another and another and another patient was carried in and laid on the floor of the already packed emergency department, and all the while in the background the tut-tut-tut-tut of machine guns and the occasional large boom from explosions that sounded way too close for comfort.
In any case, MSF had clearly ‘indicated their presence’ to both the US and Afghan authorities by providing them with the GPS co-ordinates of the Trauma Centre (see my previous discussion here). Dunlap finds this ‘commendable’ but ‘legally problematic’.
Instead, he is fixated on the absence of a Red Cross flag from the roof, in which case he might reflect on another passage from the report. On 2 October, the day before the air strike, MSF phoned the Special Operations Task Force in Bagram to develop a contingency plan: while the Taliban were respecting the neutrality of the Trauma Centre and ‘treating the government casualties well’, they wanted to know the feasibility of extracting their patients should conditions deteriorate. During that conversation they were advised to ‘take the signs normally affixed to the sides of the trucks and to install them on the top of the vehicles for easy identification by aircraft during this or any future MSF resupply operations‘ (503; my emphasis). This surely makes it clear that the US military anticipated no difficulty in recognising MSF’s flag and logo as symbols of medical neutrality.

(2) Conditional immunity
IHL makes it clear that treating wounded combatants does not compromise the protections afforded to a medical facility; that occurs only if it is used as a base from which ‘to commit, outside their humanitarian duties, acts harmful to [one of the belligerents]’. I’ll address the intervening clause – ‘outside their humanitarian duties’ – under (4) and confine my discussion here to the alleged militarisation of the clinic.

MSF’s internal review found that its unambiguous ‘no weapons‘ policy was adhered to:
All of the MSF staff reported that the no weapons policy was respected in the Trauma Centre. [Since the KTC opened, there were some rare exceptions when a patient was brought to the hospital in a critical condition and the gate was opened to allow the patient to be delivered to the emergency room without those transporting the patient being first searched. In each of these instances, the breach of the no weapon policy was rapidly rectified.] In the week prior to the airstrikes, the ban of weapons inside the MSF hospital in Kunduz was strictly implemented and controlled at all times and all MSF staff positively reported in their debriefing on the Taliban and Afghan army compliance with the no-weapon policy.
The US military investigation accepted this was indeed the case:
Evidence provided to the investigation team supports the MSF internal initial report’s characterization that their no-weapons policy was adhered to with rare exceptions (038, note 15).

Mathieu Aikins‘s interviewees also confirmed the absence of weapons from the Trauma Centre:
Though the MSF hospital was crowded with fighters, whether patients or caretakers (each patient was allowed one), staff members and civilians who were present said the insurgents respected the rules. They left their weapons outside or handed them over at the gun lockers at the entrance. One employee recalled seeing a fighter give up his weapon but forget his ammunition vest; when the employee nervously approached the fighter about it, the man apologized profusely and handed it over. “We had respect for the hospital, as they were serving the people,” said Shahid, the Taliban commander. “I myself went there once when one of our men was wounded, and before entering we submitted our weapons outside.”
Aikins goes on to report that patients were allowed to retain their cellphones, and some of their caretakers retained hand-held radios whose transmissions were intercepted by Afghan special forces. They in turn concluded that not only were the Taliban inside the hospital but were using it as a base: ‘They had raised their flag and established their headquarters there.’ On 1 October, presumably in response to these reports, the Pentagon contacted MSF in New York to ask whether ‘they had a large number of Taliban “holed up”’ in the Trauma Centre, and were assured that the only Taliban inside the hospital were wounded patients.
But the suspicions clearly remained, and festered to such a degree that some of those on the ground were convinced that the hospital had been overrun by Taliban fighters. Associated Press reported that the radio intercepts prompted US analysts to request ‘specific intelligence-gathering flights over the hospital’ – their outcome has never been disclosed – and on 1 October a senior Special Forces commander (whether in Kabul or in Kunduz is unclear) wrote in his daily log that the Trauma Centre was under Taliban control and that he planned to clear it in the coming days. At least some of the Green Berets in Kunduz agreed with his assessment: ‘They were using it as a C2 node … They had already removed and ransomed the foreign doctors, and they had fired on partnered personnel from there.’ Indeed, after the attack a senior US officer in Kabul was told – by whom has been redacted – that ‘there were three dead Military-Aged Males near the hospital, identified as Taliban by the local population. They were using the hospital as a command post (using its protected status)’ (275).
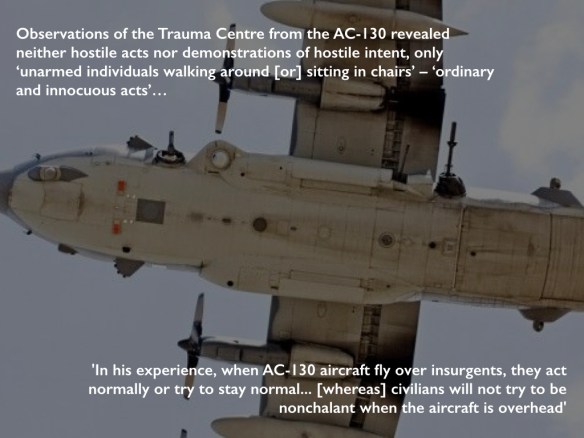
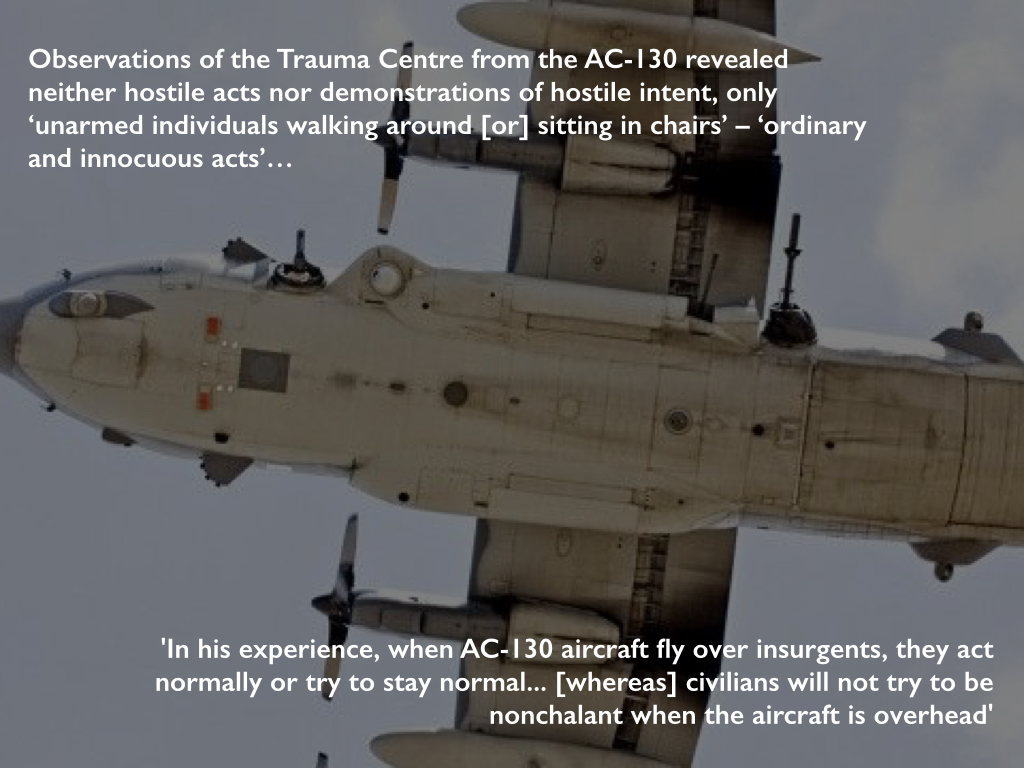
But all of this was fantasy, and the investigation discounted it. Although US intelligence reported that insurgents were present at the hospital at the time of the strike, the investigation accepted that this was for medical treatment and they could trace ‘no specific intelligence reports that confirm[ed] insurgents were using the MSF Trauma Center as an operational C2 [command and control] node, weapons cache or base of operations’ (085). In addition, they determined that observations made from the AC-130 revealed neither substantive hostile acts nor demonstrations of hostile intent – only ‘unarmed individuals walking around [or] sitting in chairs’ (085). The report describes these as ‘ordinary and innocuous acts’ (055), but to at least one member of the aircrew that was in itself grounds for suspicion: ‘In his experience, when AC-130 aircraft fly over insurgents, they act normally or try to stay normal… [whereas] civilians will not try to be nonchalant when the aircraft is overhead’ (093, note 304). Damned if you do, and damned if you don’t: when everything is construed as hostile, even the most innocent acts are transformed into somcething sinister.
The claims made by Afghan forces were even wilder. Here is May Jeong in The Intercept:
On the night of the hospital strike, a unit commander with the Ministry of Defense special forces was at the police headquarters taking fire from the direction of the hospital. “Vehicles were coming out of there, engaging, then retreating,” he told me. When I pointed out that he couldn’t have seen the gate of the hospital from where he was, several hundred meters away, he said that he was sure because he had personally interrogated a cleaner who told him that the hospital was full of “armed men using it as a cover.” The cleaner told the commander that there were Pakistani generals using the hospital as a recollection point and that they had set up a war room there. When I challenged his line of vision again, he responded, “Anyone can claim anything. The truth is different.”

[Amrullah] Saleh, [former head of the National Security Directorate and] the author of the 200-page Afghan commission report on the fall of Kunduz … believed that the “hospital sanctity had been violated” and held out as evidence 130 hours of recorded conversations with more than 600 interlocutors. “I spoke with the MSF country director,” Saleh told me recently. “They don’t deny that the hospital was infiltrated by the Taliban.”
But of course they did deny it: repeatedly, emphatically and convincingly.
(3) War crimes?
The US military investigation was unequivocal: it found multiple violations of the military’s own Rules of Engagement and of international humanitarian law.
The first rule of customary international humanitarian law, now codified in the Additional Protocols to the Geneva Conventions, is distinction:
The parties to the conflict must at all times distinguish between civilians and combatants. Attacks may only be directed against combatants. Attacks must not be directed against civilians.
The investigation found that both the Ground Force Commander (GFC) and the aircraft commander failed to exercise this core principle:
Neither commander distinguished between combatants and civilians nor a military objective and protected property. Each commander had a duty to know, and available resources to know that the targeted compound was protected property’ (075-6).
A second core principle is proportionality:
Launching an attack which may be expected to cause incidental loss of civilian life, injury to civilians, damage to civilian objects, or a combination thereof, which would be excessive in relation to the concrete and direct military advantage anticipated, is prohibited.
The investigation found this to have been disregarded too:
The GFC and the aircraft commander failed to exercise the principle of proportionality in relation to the direct military advantage (076).
Both principles are deceptively simple, and in ‘The Passions of Protection: Sovereign Authority and Humanitarian War’ Anne Orford reminds us that IHL ‘immerses its addressees in a world of military calculations.’ In practical terms the distinction between civilians and combatants in today’s conflicts is rarely straightforward, but in this case the No-Strike List plainly recognised the protected status of the Trauma Centre and there is no convincing evidence that its immunity had been compromised. In addition, the balance between loss of civilian life and military advantage is weighed on the military’s own scales – ‘expected’; ‘excessive’; ‘anticipated’: these are not self-evident calculations – but even if the GFC or the aircraft commander had grounds to believe the Taliban were firing from the hospital the Pentagon’s own Law of War Manual (which is not without its own controversies: see here and, specifically on proportionality, here and here) advises under §7.10.3.2 that
The obligation to refrain from use of force against a medical unit acting in violation of its mission and protected status without due warning does not prohibit the exercise of the right of self-defense. There may be cases in which, in the exercise of the right of self-defense, a warning is not “due” or a reasonable time limit is not appropriate. For example, forces receiving heavy fire from a hospital may exercise their right of self-defense and return fire. Such use of force in self-defense against medical units or facilities must be proportionate.
Not only was there was no evidence of hostile let alone ‘heavy fire’ from the Trauma Centre but the AC-130 was also monitoring the progress of the Afghan Special Forces convoy that it was tasked with protecting and knew perfectly well that it was still within the perimeter of the airfield. This was not a time-sensitive target (the report makes that crystal clear) and neither the GFC nor the aircraft commander had reason to believe that any putative threat to Afghan or US forces was so grave and so sustained that it called for an air strike involving multiple passes by the AC-130 – over 30 minutes according to the US military, an hour according to MSF – delivering such intense fires that the building was virtually destroyed.
For these reasons many commentators – and MSF (‘Under the clear presumption that a war crime has been committed, MSF demands that a full and transparent investigation into the event be conducted by an independent international body’) – have insisted that the attack was a war crime.


But others (including the US military) have concluded that it was not. US Central Command’s initial summary – produced before the redacted report was released – accepted that there had been breaches of both the Rules of Engagement and of IHL (‘the law of armed conflict’) but noted that
the investigation did not conclude that these failures amounted to a war crime. The label “war crimes” is typically reserved for intentional acts – intentionally targeting of civilians or intentionally targeting protected objects. The investigation found that the tragic incident resulted from a combination of unintentional human errors, process errors and equipment failures, and that none of the personnel knew that they were striking a medical facility.
The report has been so heavily redacted so that this legal discussion is unavailable (see also the commentary by Sarah Knuckey and two of her students here). We do know that the investigation team included an unnamed legal advisor from US Central Command (CENTCOM) and that its report was subject to legal review by the Staff Judge Advocate, who accepted its findings as ‘legally sufficient’ with several, redacted exceptions – though there is no way of knowing what they were (007-009). We know too that General John Campbell, who ordered the investigation as commander of US Forces in Afghanistan, subsequently disapproved a number of findings and recommendations ‘not related to the proximate cause of the strike’ (002) but, again, the details have been excised.

General Joseph Votel, commander of CENTCOM, repeated the summary statement’s disavowal of war crimes at a Pentagon Press Briefing on 29 April 2016, and in responding to a storm of questions from plainly incredulous reporters (above) he elaborated:
… an unintentional action takes it out of the realm of actually being a deliberate war crime against persons or protected locations…. They were absolutely trying to do the right thing; they were trying to support our Afghan partners; there was no intention on any of their parts to take a short cut, or to violate any rules that were laid out for them. And they were attempting to do the right thing. Unfortunately, they made a wrong judgment in this particular case…
Jens David Ohlin explains the disputation (which Faye Donnelly helpfully re-casts as one between two contending narratives whose speech-acts struggle to realize their performative force):
The problem is that the killing of the innocent civilians was not intentional, it was accidental. As a matter of criminal law, it was either reckless or negligent … but the civilian killings were not performed with purpose.
The Rome Statute of the International Criminal Court provides for war crimes prosecutions for ‘intentionally directing’ or ‘intentionally launching’ attacks that contravene international humanitarian law (in effect, criminalizing the rules of IHL). Jens discusses this in relation to attacks on civilians, but the Statute also proscribes ‘intentionally directing attacks against buildings, material, medical units and personnel’ or against ‘personnel, installations, material, units or vehicles involved in a humanitarian assistance or peacekeeping mission’.
In every case the emphasis is on intentionality, and yet intentionality – as philosophers have demonstrated time and time again – is not the simple, settled matter some legal scholars assume it to be. Jens’s central point is that common-law cultures identify intentionality with purpose or knowledge whereas civil-law cultures widen its sphere to include a conscious disregard of risk or ‘recklessness’. The full argument is here – including an intricate disection of the (geo)politics involved in drafting the Geneva Conventions and the Additional Protocols – but the sharp conclusion is that (for Jens, at least) the strike on the Trauma Centre would not constitute a war crime under the first count (he accepts that neither the GFC nor the aircraft commander possessed the knowledge or the purpose) but could under the second (their actions, and those of others, were reckless). I should add that he recommends the recognition of a new war crime to explicitly address the second count and thereby signal ‘the moral difference between intentionally killing civilians and recklessly killing them.’
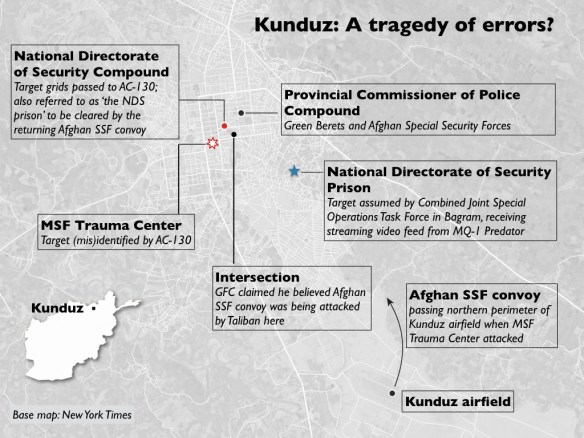
The investigation report provides endless, explicit examples of a thoroughly compromised ‘risk management process’ by multiple actors at multiple sites, and this dispersal of responsibility in Kunduz (see map above) and Bagram further complicates the legal situation. Peter Margulies – who does not accept that ‘the lack of intent among US personnel is determinative’ – concedes that ‘the cascading systemic errors in the hospital attack impede the attribution of culpable awareness to one or more specific individuals.’ In his view,
CENTCOM would have been better served by acknowledging that intent was not required [for the commitment of a war crime], but that awareness of risk was distributed among many organizational components, without full awareness concentrated in one or more individuals who could be charged criminally.
Adil Ahmad Haque notes that Additional Protocol I to the Geneva Conventions requires attackers to do ‘everything feasible’ to verify that their target is a military objective and instructs them in cases of doubt to presume that it is civilian – the Law of War Manual doesn’t follow this standard, but the investigation report does – and here there is such clear evidence of recklessness on the part of many of the US forces involved (whose evidence is shot through with technical failures and radical uncertainty) that, in his view, their decision to press on with the attack ‘was unlawful, irrespective of their good faith.’
(4) Medical neutrality at risk
I noted above that hospitals only lose their protected status if they are used ‘to commit, outside their humanitarian duties, acts harmful to [one of the belligerents]’. It’s a telling provision because its intermediate clause can be read as a tacit acknowledgement that those humanitarian duties – treating the sick and wounded – could otherwise be construed as acts harmful to their enemies.
And there is evidence that this is exactly how both the Afghan government and its military viewed MSF’s activities. When Mathieu Aikins visited Kunduz after the air strike he reported:
Some members of the Afghan government and security forces there had little respect for MSF’s neutrality and resented its treatment of wounded Taliban. When I visited Kunduz in November, their anger was still surprisingly raw, despite the recent destruction of the hospital. “They give them medicine; they transport and treat their injured,” [Colonel Abdullah] Gard, the commander of the [Ministry of Interior’s] quick-reaction force, told me. “Their existence is a big problem for us…. The people that work there are traitors, all of them.”

Gard (seen above) and one of his colleagues told May Jeong exactly the same:
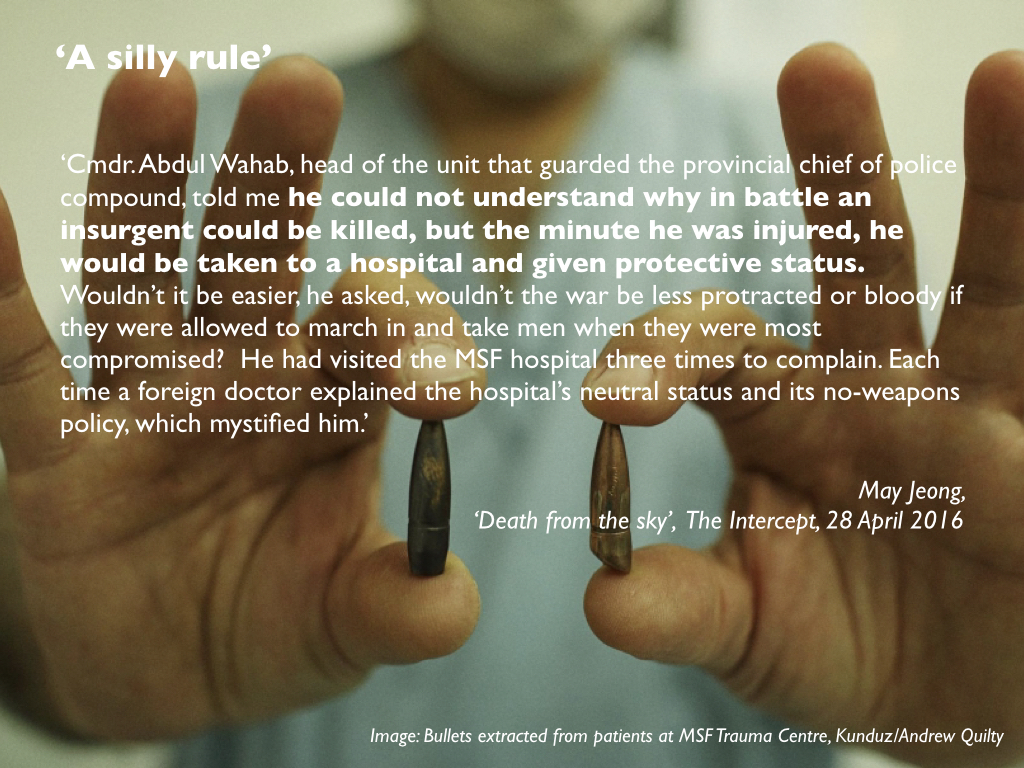
Gard spoke of MSF with the personal hatred reserved for the truly perfidious. He accused the group of “patching up fighters and sending them back out,” a line I heard repeatedly. Cmdr. Abdul Wahab, head of the unit that guarded the provincial chief of police compound, told me he could not understand why in battle an insurgent could be killed, but the minute he was injured, he would be taken to a hospital and given protective status. Wouldn’t it be easier, he asked, wouldn’t the war be less protracted or bloody if they were allowed to march in and take men when they were most compromised? He had visited the MSF hospital three times to complain. Each time a foreign doctor explained the hospital’s neutral status and its no-weapons policy, which mystified him.
In short, it seems that some (perhaps many) in the Afghan security forces – particularly after the humiliation of being forced out of Kunduz – believed that the Taliban were legitimate targets wherever they were and that the fight against them was being hamstrung by what one officer described to Jeong as a ‘silly rule’.

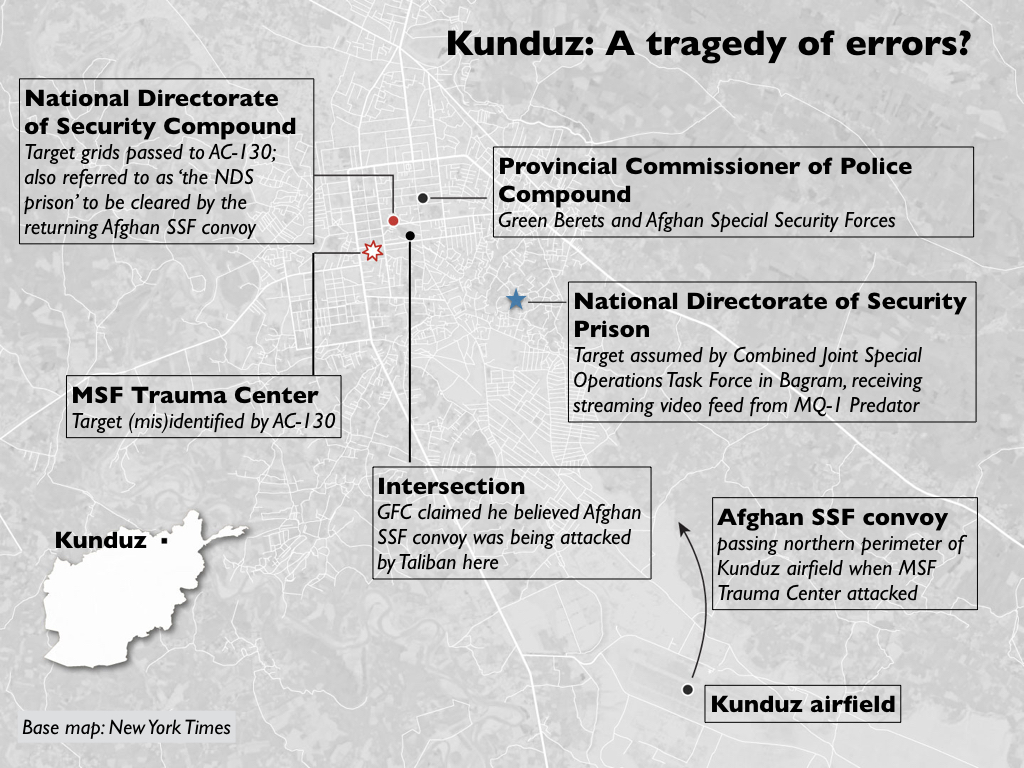
This becomes material because, as I showed previously, the intended target for the air strike was a National Directorate of Security compound whose co-ordinates had been passed to Major Michael Hutchinson, the Ground Force Commander, by Afghan Special Security Forces (who, like him, were unfamiliar with the city): they had identified the NDS compound as a Taliban command and control node, and planned to clear it on their return from the airfield following a casualty evacuation. The AC-130 was supposed to provide Close Air Support, but a series of technical difficulties compromised the accuracy of its sensors and several hours after the Afghan Special Security Forces had left in an armoured convoy with their three casualties the aircrew were still unsure of the location of the target and so requested a verbal description of the NDS compound. This was provided by Afghan forces still inside the Provincial Chief of Police compound: their description matched the MSF Trauma Centre much more closely than the NDS compound, and the aircrew fixed on this as their target.
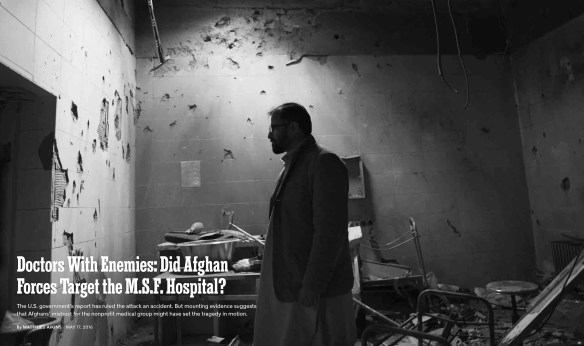
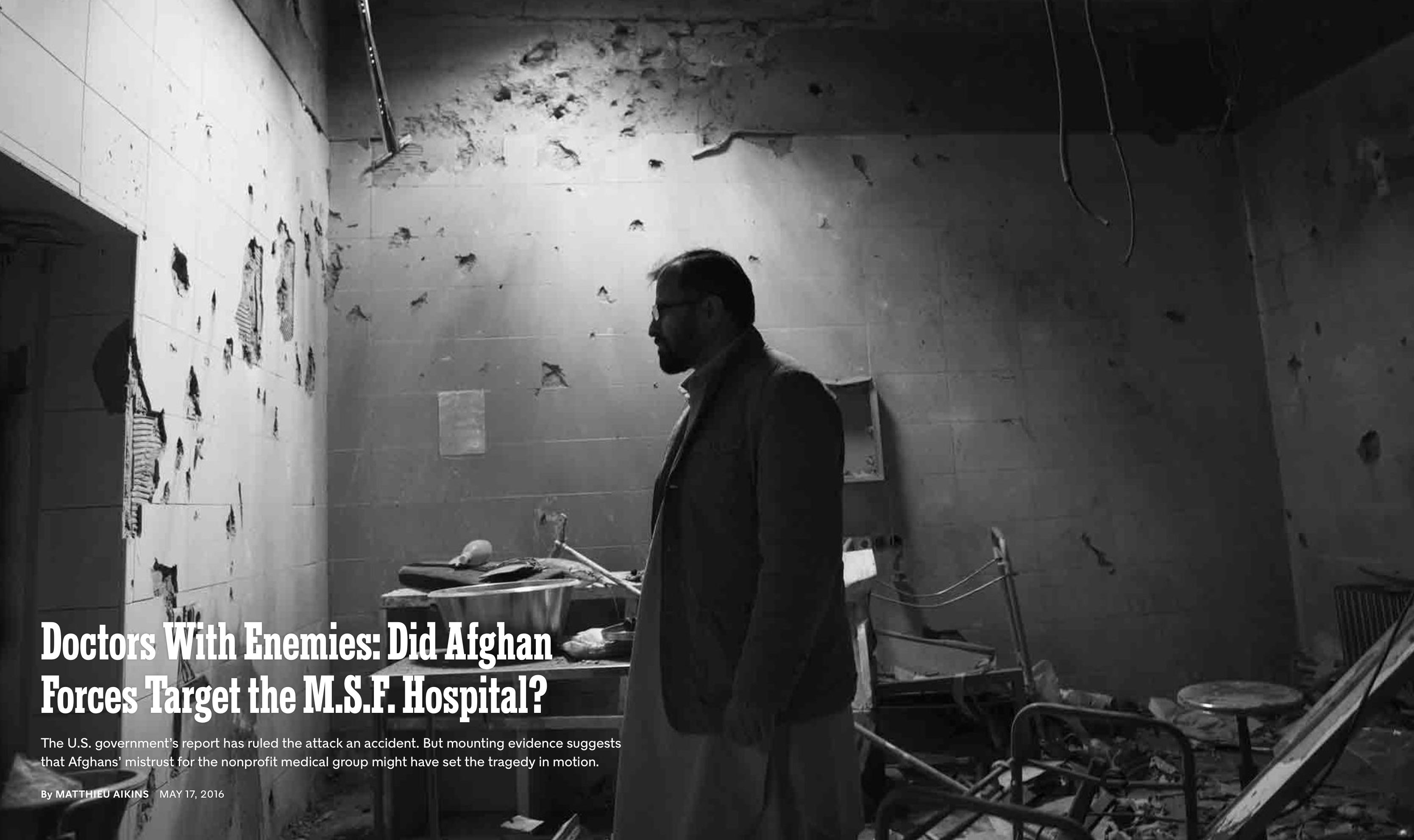
It’s impossible to know whether this was a mistake or misdirection, and the report fails to identify who provided the description. Hutchinson was shown various photographs but explained that ‘it was dark when everything happened’; he couldn’t remember the name of the Afghan liaison officer and – the redactions make his responses difficult to follow at this point – he wasn’t always sure who he was talking to since he had to rely on interpreters (387-8). But the description obviously had to come from someone who knew the city (which would include Gard and Wahab), and both Aikins and Jeong clearly believe that misdirection is not only possible but also extremely likely. ‘That hospital is in the service of the Taliban,’ Gard told Aikins. ‘I swear to God, if they make it a hundred times, we’ll destroy it a hundred times.’ Hence the headline for Aikins’s searching New York Times report (above): ‘Doctors with enemies: did Afghan forces target the MSF hospital?‘ I should note that David Glazier dismisses all this as ‘highly speculative’ and insists that ‘it simply defies logic’. While the claim is speculative it surely doesn’t defy logic, and Aikins and Jeong make at least a plausible if not definitive case). They are clearly not alone in their suspicions: MSF’s very first question in response to the investigation report was this:
‘What was the physical description of the intended target provided by the Afghan forces and how did it match the description of the MSF hospital?’

The studied refusal to recognise medical neutrality – if that is what this was – emerges from a long history of friction between MSF and the government in Kabul, and it threads its way out into a wider history and geography of deliberate attacks against medical facilities elsewhere in Afghanistan, and – among other recent places – in Gaza (by the Israeli military), in Syria (primarily by the Russian and Syrian Arab Air Forces) and in Yemen (primarily by the Saudi-led coalition which is advised by the United Kingdom on targeting). In February 2014 Thanassis Cambanis was already writing that ‘medical care is now a tool of war’, and in a report issued in May 2016 the World Health Organisation counted almost 600 attacks against medical facilities, doctors and nurses in 19 countries since then. These shocking statistics, which are inevitably imperfect, include attacks by non-state actors, among them the Taliban and Islamic State, but I have emphasised the complicity of state actors – including leading members of the UN Security Council – because it is their actions that determine the course of international humanitarian law and because they are ultimately responsible for what MSF’s president Joanne Liu saw in the wake of the attack on its Trauma Centre in Kunduz as ‘not just an attack on our hospital’ but ‘an attack on the Geneva Conventions.’

In a letter to the UN Security Council issued on 22 September 2016, after a direct and deliberate attack on a humanitarian convoy delivering aid to eastern Aleppo, more than 100 humanitarian organisations noted that:
‘Each [head of state] that accepts a lack of accountability for perpetrators and facilitators of war crimes colludes in the ongoing dissolution of international humanitarian law.’
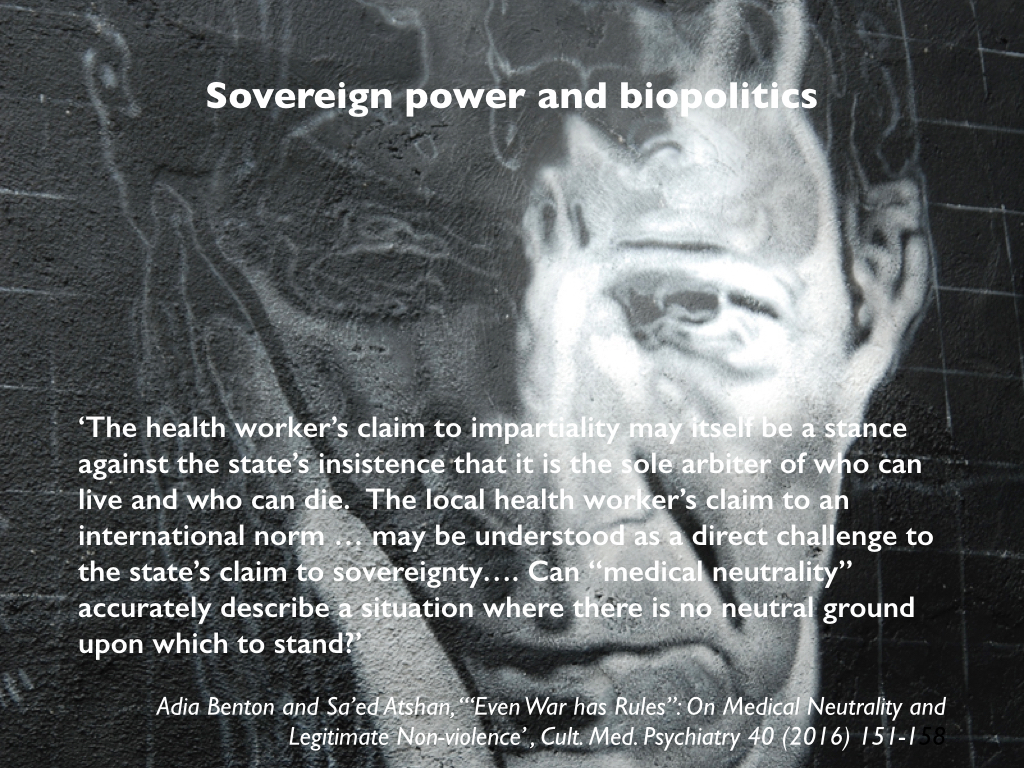
That dissolution can be seen as a defiant reassertion of the absolutism of sovereign power, because ‘medical neutrality’ is not a neutral claim. Adia Benton and Sa’ed Ashtan persuasively argue that:
The health worker’s claim to impartiality may itself be a stance against the state’s insistence that it is the sole arbiter of who can live and who can die. The local health worker’s claim to an international norm … may be understood as a direct challenge to the state’s claim to sovereignty…. Can ‘‘medical neutrality’’ accurately describe a situation where there is no neutral ground upon which to stand? (‘‘‘Even War has Rules’’: On Medical Neutrality and Legitimate Non-violence’ , Cult. Med. Psychiatry 40 (2016) 151-158).
As the spectral presence of Giorgio Agamben in my slide below implies, this has the liveliest implications for how we are to understand the space of exception and the refusal of its victims to be reduced to the passivity of ‘bare life’.
As I will show in the next post in this series, Syria is the most egregious contemporary case. If some members of the Afghan security forces wilfully misled the Americans into targeting the MSF Trauma Centre in Kunduz, then it seems clear that they objected to the protection extended by IHL to wounded Taliban combatants and those who treat them (though many of those killed in the attack were civilians, despite Alan Dershowitz‘s tawdry attempt to suggest that MSF ‘favoured Taliban fighters over civilian patients’: see Kevin Jon Heller’s magisterial response here). But in Syria not only has the provision of medical aid to those in rebel-held areas been explicitly criminalised by the state’s new Counterterrorism Law which came into effect in July 2012 – the space of exception is far from being a ‘legal “black hole” – but the ban extends to those providing medical aid to sick or wounded civilians. And make no mistake: there have been no mistakes. The murder of doctors and nurses and the bombing of hospitals and clinics in Syria has been deliberate and systematic. The exception to the exception contracts to its vanishing point.
To be continued.