One of the cardinal principles informing modern casualty evacuation is the Golden Hour. In 1975 R. Adams Cowley, founder of Baltimore’s Shock Trauma Institute, argued that ‘the first hour after injury will largely determine a critically injured person’s chances for survival.’ It’s not a straightforward metric, and combat medical care and evacuation has been transformed since it was first proposed, but the rule of thumb is that the chances of survival are maximised if the time between traumatic injury and definitive care is kept to 60 minutes or less.
Following a fire-storm of criticism on 15 June 2009 US Secretary of Defense Robert Gates required the standard time between a call for evacuation and treatment of the critically injured to be 60 minutes or less. For US military personnel in the Second World War the average time was 10 hours; in Korea that had been cut to 5 hours (the result of using helicopters for speedy evacuation); and in Vietnam it was already down to one hour. The reason for Gates’s intervention was that in Afghanistan the aim was two hours…

U.S. Air Force Sgt. Daniel Fye serving on a tour in the Kandahar province of Afghanistan in April 2011. (Courtesy of Daniel Fye)
The importance of those time-critical sixty minutes was no secret to the troops in the line of fire. Here is a scene from Brian Castner‘s truly brilliant All the ways we die and kill which imagines the thoughts running through one soldier’s head – Air Force Technical Sergeant Dan Fye on his third tour of duty with Explosive Ordnance Disposal (above) – after he stepped on an IED during a clearance operation in Mushan (Panjwayi) on 27 May 2011:
They worked on Fye a long time, and the longer they worked, the more anxious Fye got about the precious minutes slipping away. “I don’t hear the bird,” he said, over and over. They wrote the time of the tourniquet application on the white headband Fye wore under his helmet. Hopkins pushed morphine into his veins.
Eventually, an eon since Hopkins arrived but only twenty-five minutes after the blast, the hyperactive thump of helo blades cutting air slowly emerged in the distance.
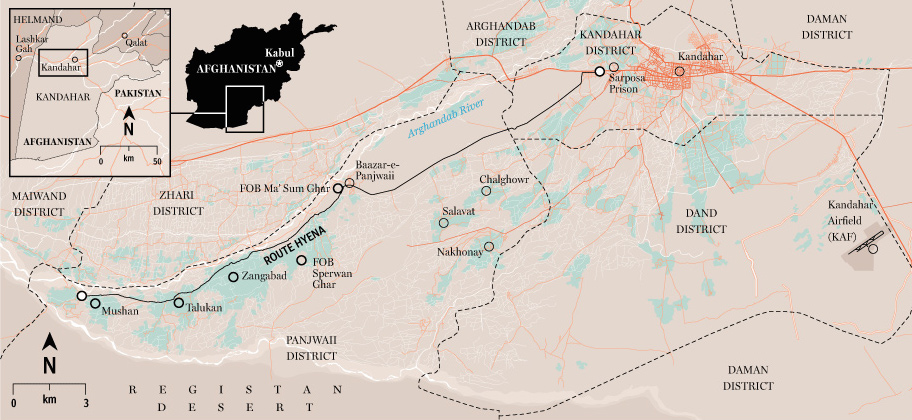
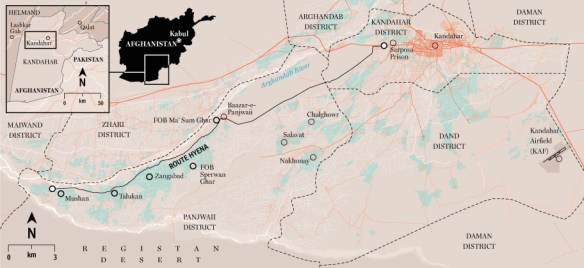
Fye thought it was the most wonderful sound he had ever heard. They were at the extreme limit of the NATO footprint, and so it was a sixty-kilometer flight to the main hospital at Kandahar [see map below]. If they moved quickly, Fye would just make it in the magic golden hour.
Castner writes that as Fye was bleeding out in the back of the helicopter, he was
‘clinging to one thought and one thought only, running in a continuous Times Square news ticker across the front of his oxygen-starved brain: One hour. If I can get back to Kandahar in one hour, I’ll live. One hour, and I’ll live. That’s what they say. You’ll make it if you can get back to the hospital in one hour.’
He made it. The new, modernised and expanded Role 3 NATO hospital at Kandahar had opened a year earlier, and its executive officer claimed that ‘They hit our doors, they live.’
But Fye was lucky. Later he learned why it had taken so long for the helicopter to arrive, and why he very nearly never made it to Kandahar at all:
Over multiple radio calls between Hopkins’s platoon and the rescue operations center, his report of “bilateral amputation” had been converted, telephone-game style, into “bilateral lacerations.” The medical operations center had actually turned the rescue mission off; helos don’t fly for scraped knees. The bird that eventually picked up Fye wasn’t even a real medevac bird. That’s why the robotic flight crew ignored him, didn’t treat his wounds as they went. They weren’t medics. The helo pilots had just been in the air and happened to overhear the radio traffic, including the original call for help. They understood the mistake and had disobeyed orders to go get Fye. If the human pilot of that bird had been less stubborn, the golden hour would have been long past by the time Fye made it to KAF, and he could well have been one of the 1 percent.
(More from Brian on medical evacuation here and here).
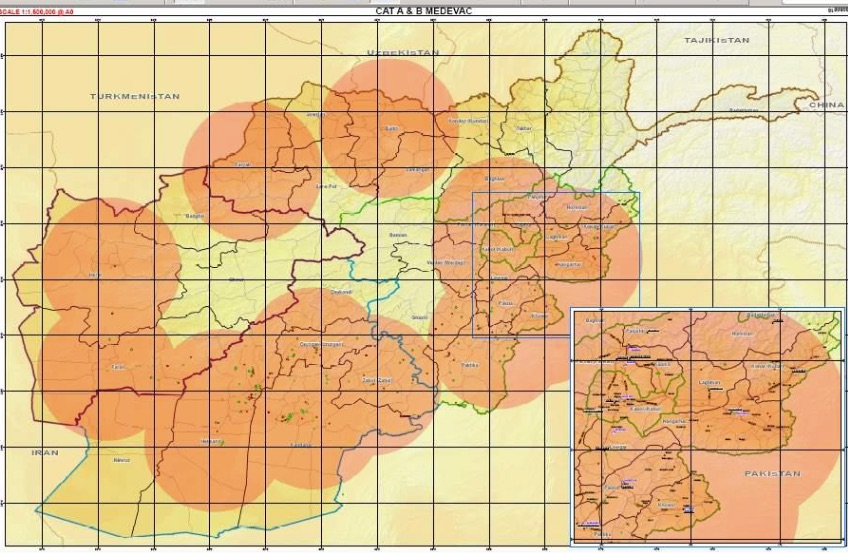
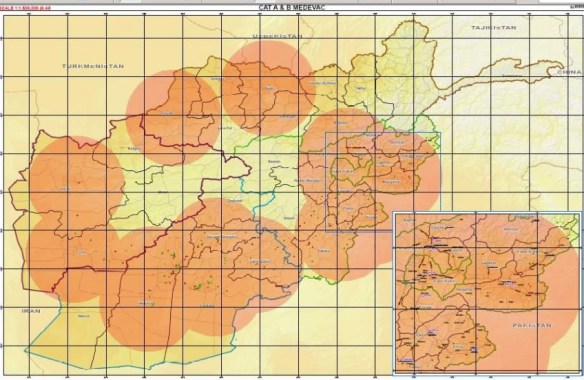
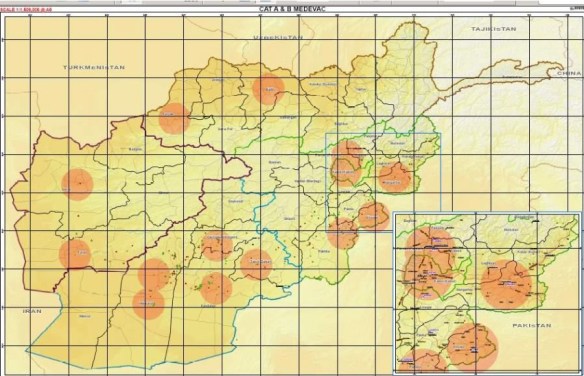
Even without miscommunication the logistical challenges were formidable. In 2007, two years before Gates’ intervention, ISAF produced this map showing the medevac coverage – what Fye called the ‘NATO footprint’ – that supported that two-hour standard (I have taken this map and the following one from a report prepared by Col Dr Ingo Hartenstein for NATO/ISAF in December 2008 which is available here; scroll down):
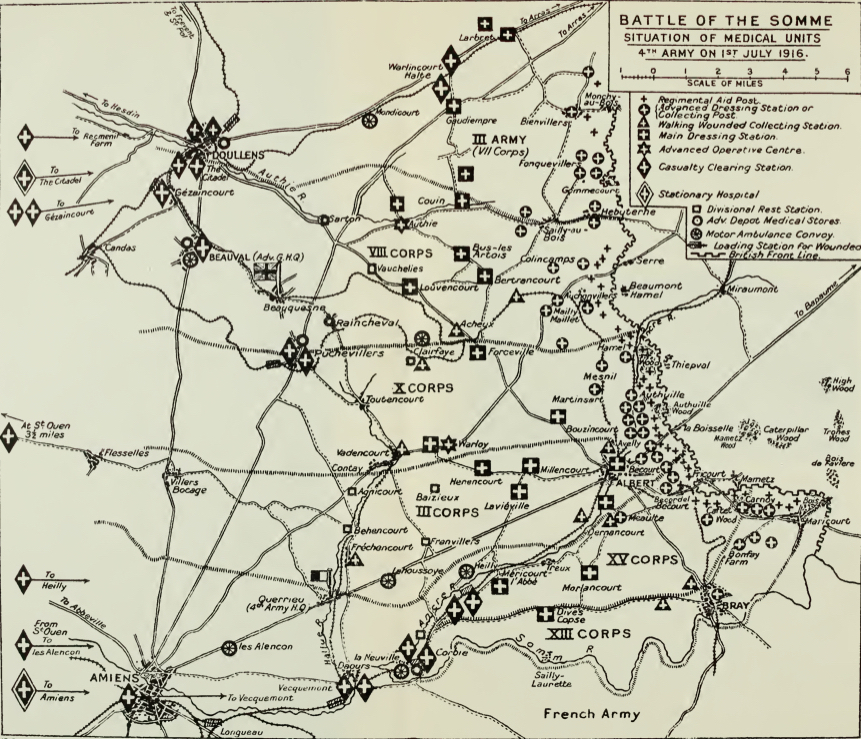
Like Vietnam, Afghanistan was a ‘war without fronts’ with a battlefield geometry that imposed a radically different evacuation model from the classical line of evacuation that had been established during the First World War. Here is how Brian Turner puts it in My life as another country:
We won’t hear the battle in progress and work our way toward it as baggage trains of wounded, exhausted soldiers and civilians carrying their lives on their backs travel in the opposite direction. Our battle space – and perhaps it’s a cliché now – will occur in a 360-degree, three-dimensional environment.
More technically, here is Brigadier Martin Bricknell, who served (among many other roles) as Medical Adviser to ISAF’s Regional Command South in Kandahar in 2010:
The tactical geometry for the current operating environment is based upon security forces holding areas of ground and securing this space from opposition activity. This converts the battlefield from the conventional force-on-force linear geometry with an identifiable confrontation line to an area battlefield with multiple nodes of contested space. Thus the MEDEVAC mission is converted from a linear flow to area support, hence MEDEVAC planning is based upon a ‘range ring’ coverage with a radius of 40–60 nautical miles.
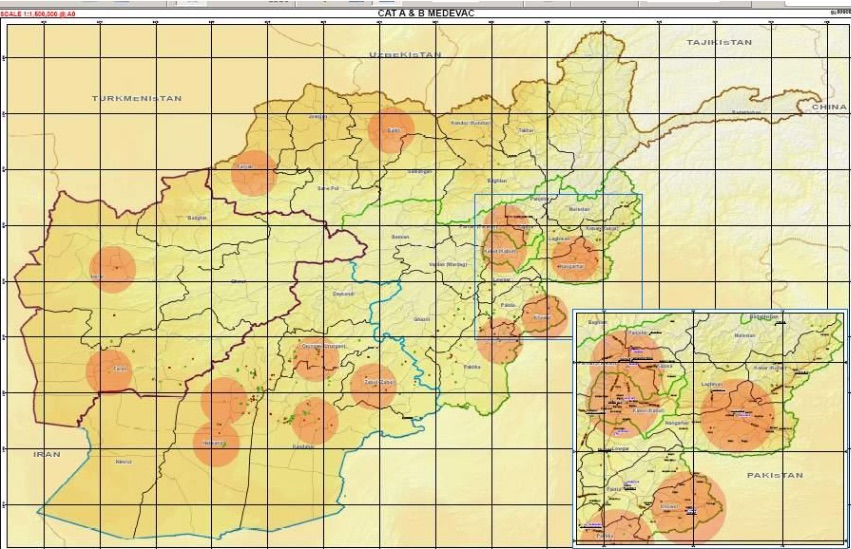
Given the available resources, a second map showed how those ‘range rings’ would contract if the Golden Hour were to be imposed over the evacuation grid:
In practice, the situation was more variable than these maps imply – not least because there was a significant difference between the ways in which American and British contingents organised medical evacuation.
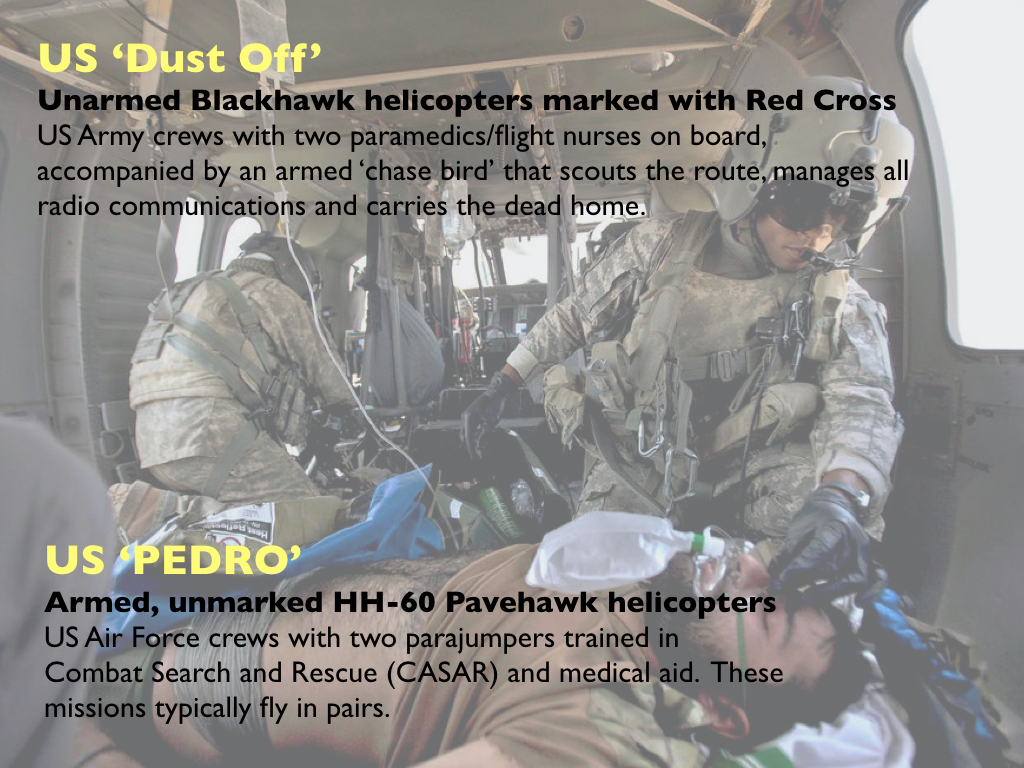
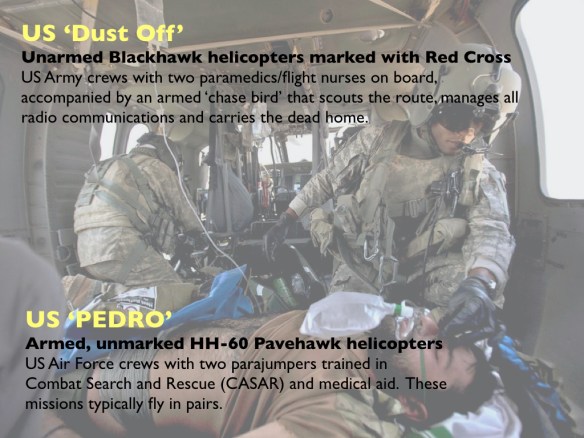
The US military, drawing on their experience in Vietnam, used Blackhawk or Pavehawk helicopters to get paramedics or combat medical technicians to the casualty as fast as possible:

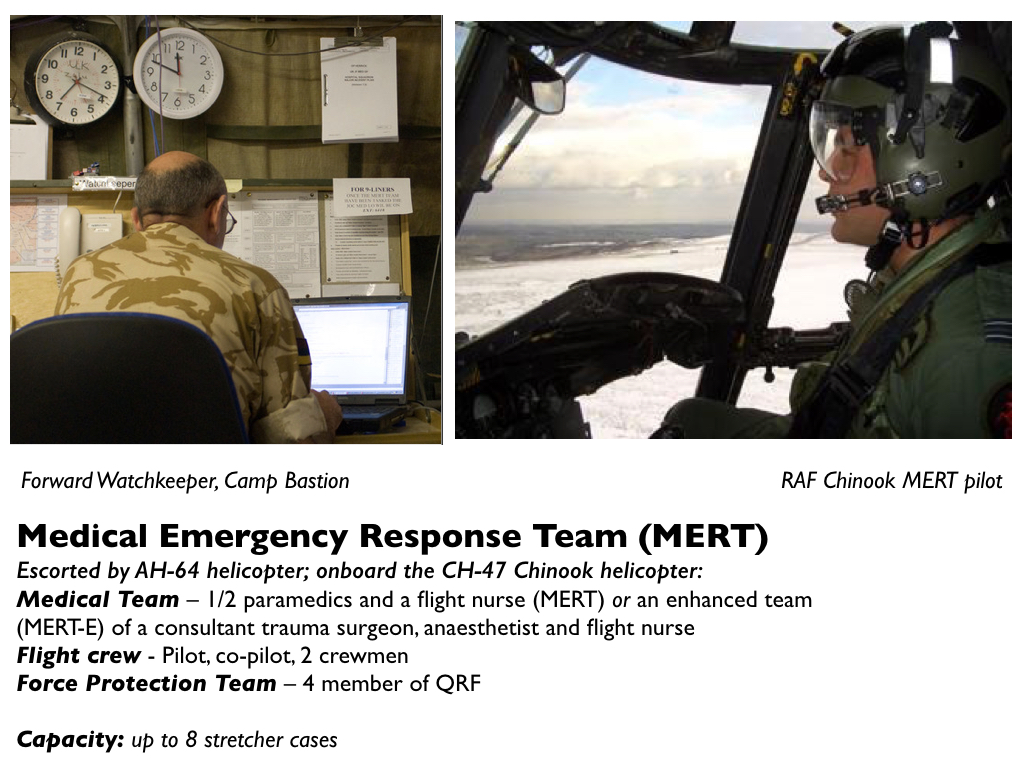
The British used larger Chinook helicopters to dispatch a Medical Emergency Response Team (MERT) with a trauma surgeon onboard to the casualty close to the point of injury (POI):
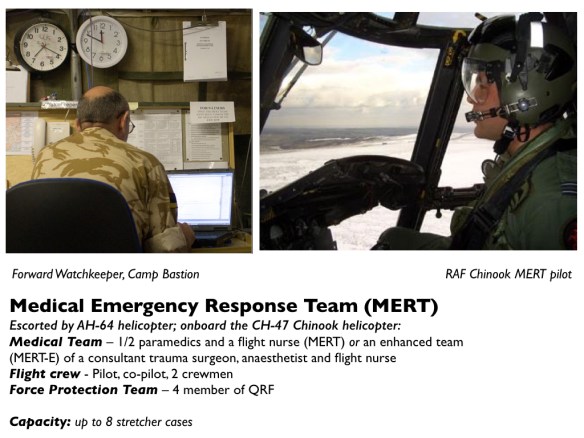
The response time was usually longer but the MERT enabled advanced trauma care to begin as soon as the patient was onboard.
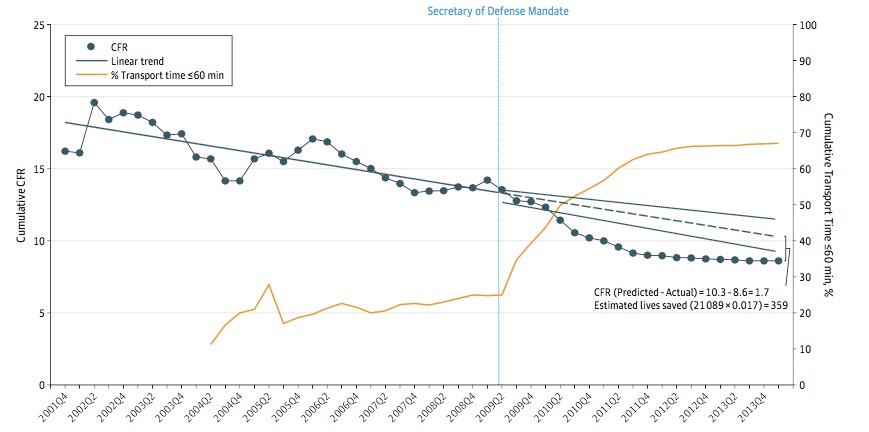
There has been considerable debate and disagreement about the robustness of the ‘Golden Hour’ in military trauma care and its relation to evacuation pathways: see, for example, Jonathan Clarke and Peter Davis, ‘Medical evacuation and triage of combat casualties in Helmand Province, Afghanistan: October 2010-April 2011’, Military Medicine 171 (11) (2012) 1261-6. But a research team has now calibrated the effects of reduced evacuation time on US casualty fatality rates (CFR) in Afghanistan between 2001 and 2014 [Russ Kotwal et al, ‘The effect of a Golden Hour policy on the morbidity and mortality of combat casualties’, JAMA Surgery 151 (1) (2016) 15-24; see also here]:
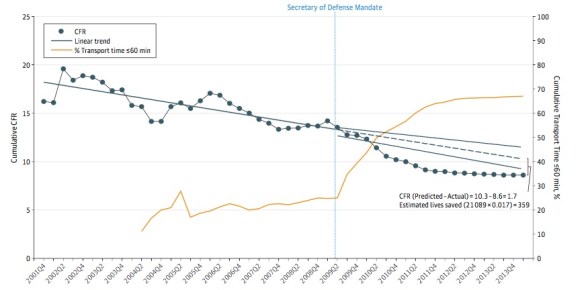
For 4,500 cases of US military casualties with detailed data the study showed a substantial change in the CFR following the Secretary of Defense’s mandate to evacuate casualties within 60 minutes: as the median evacuation time fell from 90 minutes to 43 minutes the CFR fell from 13.7 to 7.6; before the mandate 25 per cent of casualty evacuation missions fell within the Golden Hour, after the mandate the proportion soared to 75 per cent.
The interpretive field is a complicated one – while a significant number of casualties who would previously have died from their wounds now survived, a proportion of those who would previously have been recorded as ‘killed in action’ (KIA) none the less now ‘died of wounds’ (DOW) – and the reasons for the improvement in survival rates are also multivariate:
‘Secondary effects resulting from the mandate that contributed to achieving the mandated time included stream-lined authority and helicopter launch procedures, increased number and dispersion of Army helicopters, and the addition of Air Force helicopters to assist with the Army prehospital transport mission. As decreased time from critical injury to treatment capability was the underlying goal, personnel with increased expertise (blood transfusion protocol-trained basic medics, critical care paramedics, and critical care nurses) were trained and assigned to prehospital flights more routinely, resulting in earlier availability of blood products and other advanced care.
In addition, an increase in the number and dispersion of small but mobile forward surgical teams across the battle-field brought major surgical capability even closer to the point of injury and provided an alternative to transporting patients longer distances to large, but less mobile, civilian trauma center–equivalent [Combat Support Hospitals].’
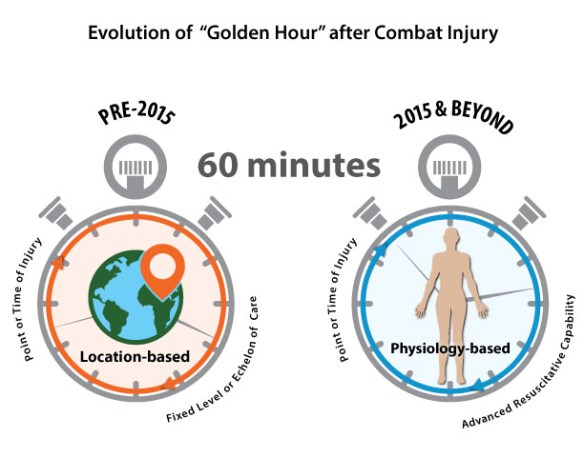
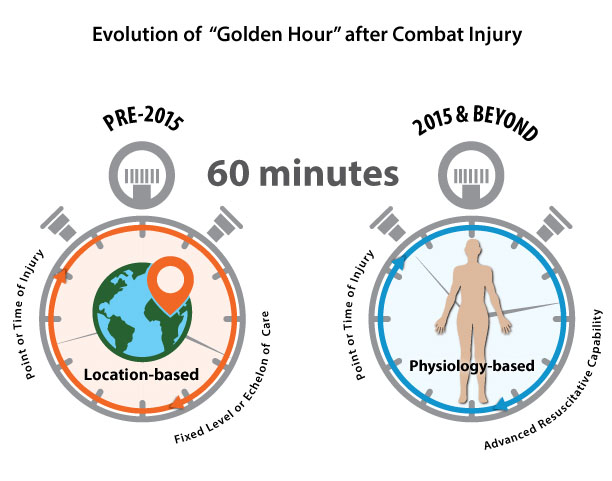
These findings – together with the experience of the British MERTs – intersect with a recalibration of the Golden Hour. The US Combat Casualty Care Research Program (CCCRP) has proposed an ‘evolved concept’ (see the figure above) that moves from a location-based protocol to a physiological one:
The program must be willing to turn the doctrine of fixed or traditional echelons of care on its side and innovate for scenarios in which Level II and III care is performed aboard transport vehicles (land-, air- or sea-based) or within local structures of opportunity. In such circumstances, field care may be prolonged, lasting for days or even weeks. Combat casualty care research with these complex scenarios in mind promises to enhance resuscitative capability for injured service personnel regardless of environment, leveraging communications networks (i.e., telementoring) and targeted resupplies of materials. In the future, CCCRP must focus on transforming the concept of the golden hour into one bound not by the time to reach traditional echelons of care or fixed facilities, but the time until enhanced resuscitative capability can be delivered to the injured troop, regardless of location or need for transport.
There are two riders to add. First, embedded within the Golden Hour are ‘the platinum ten minutes’: the imperative to stop bleeding (which has led to the re-emergence and re-engineering of the tourniquet) and to control the casualty’s airway within 10 minutes of wounding.
The second is that the speed of treatment and trauma care available to American and British soldiers is radically different from that available to Afghan soldiers and police officers. Previously, they could rely on aeromedical evacuation by their allies. But now most of their medical evacuations take place by land, over difficult and dangerous roads. Last September Josh Smith reported:
Under the dim light of a single bulb, a local Afghan policeman lay severely injured, slipping in and out of consciousness. A military doctor reported to an Afghan army brigade commander that the man was unlikely to live through the night.

Despite the doctor’s pleas, the commander stood firm. The army could not spare any soldiers or ambulances [below] to make the five-hour drive to a better hospital at that late hour through territory teeming with Taliban ambushes and roadside bombs.

The lack of speedy evacuation is a tragically common problem for the rising number of Afghan police and soldiers being injured on the battlefields of Afghanistan. U.S. advisers have worked to help close the capability gap, but mostly behind the scenes, far from the battlefields where many Afghan troops say they increasingly feel alone.
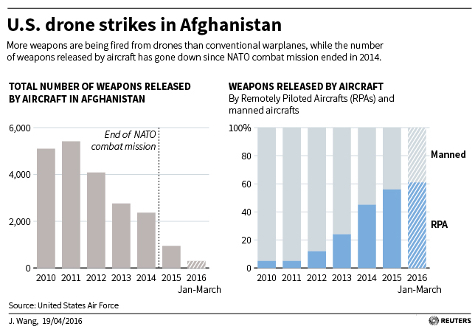
Although the American forces still stationed in the country have conducted more than 200 airstrikes since their combat mission was declared over at the end of 2014, as of July, U.S. military aircraft had not flown a single conventional medical evacuation mission, according to data released by the U.S. Air Force Central Command.
U.S. military officials say they haven’t flown evacuation missions because they haven’t been asked. Also, there are far fewer American resources available for such missions now.
The difference shows up in the ratios of those killed and those who survived their wounds.
About 2,363 Americans have died in Afghanistan, with a little more than 20,000 wounded, a ratio of roughly 1-to-10. In the first half of 2015 alone, 4,302 Afghan soldiers and police were killed in action and 8,009 more were wounded, a ratio of about 1-to-2.
Even where aircraft and trained medical technicians are available, Jeff Schogol found that the Afghan capability falls well outside the Golden Hour:
The time it takes to fly patients to hospitals varies depending on the point of injury, but it can take between 90 minutes and two and a half hours to fly an aeromedical evacuation mission in a C-208, plus one hour to transfer patients from Kandahar to Kabul in a C-130.

And the situation for Afghan civilians – as I explored in detail in ‘The prosthetics of military violence‘ – is still worse.
This is not a problem confined to Afghanistan: think of how the possibility of the Golden Hour recedes in urban combat zones subjected to artillery fire and bombing – the difficulties faced by first responders in Gaza or in the ravaged, rubble-strewn towns and cities of Syria (see also Annie Sparrow‘s report here).

A Syrian youth walks past a destroyed ambulance in the Saif al-Dawla district of the war-torn northern city of Aleppo on January 12, 2013. An accident and emergency centre in Aleppo uses an abandoned supermarket to conceal a fleet of 16 ambulances, just 10 of which are in working order and are driven by 22 staff members. AFP PHOTO/JM LOPEZ/ (Getty Images)
And there is no guarantee of safety even once casualties reach hospital since the principle of medical neutrality is now being routinely and systematically violated.